You might also like
- Microbiology for Surgical Infections: Diagnosis, Prognosis and TreatmentFrom EverandMicrobiology for Surgical Infections: Diagnosis, Prognosis and TreatmentKateryna KonNo ratings yet
- Effect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialDocument7 pagesEffect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialKirsten HartmanNo ratings yet
- The Challenge of Prognostic Markers in Acute Pancreatitis: Internist 'S Point of ViewDocument9 pagesThe Challenge of Prognostic Markers in Acute Pancreatitis: Internist 'S Point of ViewGdfgdFdfdfNo ratings yet
- Per-Protocol Repeat Kidney Biopsy Portends Relapse and Long-Term Outcome in Incident Cases of Proliferative Lupus NephritisDocument11 pagesPer-Protocol Repeat Kidney Biopsy Portends Relapse and Long-Term Outcome in Incident Cases of Proliferative Lupus Nephritisjose pablo quero reyesNo ratings yet
- Buck 2011Document9 pagesBuck 2011siti hanifahNo ratings yet
- 2018 Article 2099Document10 pages2018 Article 2099igariok06No ratings yet
- Geleris 8Document8 pagesGeleris 8Fernando GómezNo ratings yet
- Jama Li 2020 Oi 200065Document11 pagesJama Li 2020 Oi 200065Jheny LopezNo ratings yet
- Mortality and Overall and Specific Infection Complication Rates inDocument11 pagesMortality and Overall and Specific Infection Complication Rates inKarla LapendaNo ratings yet
- Independent Risk Factors of Acute Kidney Injury Among Patients Receiving Extracorporeal Membrane OxygenationDocument8 pagesIndependent Risk Factors of Acute Kidney Injury Among Patients Receiving Extracorporeal Membrane OxygenationFreddy Shanner Chávez VásquezNo ratings yet
- 10 1001@jama 2020 10044Document11 pages10 1001@jama 2020 10044Rodrigo Ehécatl Torres NevárezNo ratings yet
- Ruan2020 Article ClinicalPredictorsOfMortalityDDocument3 pagesRuan2020 Article ClinicalPredictorsOfMortalityDntnquynhproNo ratings yet
- Pancreatology: SciencedirectDocument7 pagesPancreatology: SciencedirectLea CisnerosNo ratings yet
- Sofa ScoreDocument6 pagesSofa ScoreNadiah Umniati SyarifahNo ratings yet
- Acute Respiratory Failure Due To Pneumocystis Pneumonia: Outcome and Prognostic FactorsDocument8 pagesAcute Respiratory Failure Due To Pneumocystis Pneumonia: Outcome and Prognostic FactorszikryauliaNo ratings yet
- Lay Field 2014Document11 pagesLay Field 2014chenth3r3No ratings yet
- Development and Validation of A Nomogram Using On Admission Routine Laboratory Parameters To Predict In-Hospital Survival of Patients With COVID-19Document23 pagesDevelopment and Validation of A Nomogram Using On Admission Routine Laboratory Parameters To Predict In-Hospital Survival of Patients With COVID-19dariusNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Covid 19Document9 pagesCovid 19MonicaNo ratings yet
- Clinicopathological Characteristics of 8697 Patients With COVID-19 in China A Meta-AnalysisDocument11 pagesClinicopathological Characteristics of 8697 Patients With COVID-19 in China A Meta-AnalysisBenaya PhNo ratings yet
- CT Manifestations of Coronavirus Disease 2019 A RDocument5 pagesCT Manifestations of Coronavirus Disease 2019 A ReugeniaNo ratings yet
- WJCCM 10 22Document14 pagesWJCCM 10 22Syawaluddin sakti maulanaNo ratings yet
- Post Operative PancreatitisDocument7 pagesPost Operative PancreatitisNirajan SubediNo ratings yet
- Pi Is 0140673620326568Document12 pagesPi Is 0140673620326568Mada Dwi HariNo ratings yet
- Indicación RelaparotomiaDocument6 pagesIndicación RelaparotomiaJohnHarvardNo ratings yet
- Espondilodiscitis Infecciosa Por Patógenos Poco ComunesDocument5 pagesEspondilodiscitis Infecciosa Por Patógenos Poco ComunesOthoniel RamirezNo ratings yet
- The Female Predominant Persistent Inmune Dysregulation of The Post Covid Syndrome - Ganesh - 2021Document11 pagesThe Female Predominant Persistent Inmune Dysregulation of The Post Covid Syndrome - Ganesh - 2021Isis StoreNo ratings yet
- A Simple Prognostic Score For Risk Assessment in Patients With Acute PancreatitisDocument6 pagesA Simple Prognostic Score For Risk Assessment in Patients With Acute PancreatitisGeorgiana CrisuNo ratings yet
- Effect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-AnalysisDocument36 pagesEffect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-Analysisrista ria ariniNo ratings yet
- Journal of Critical CareDocument5 pagesJournal of Critical CareUnomoshNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- !6-Month Consequences of COVID-19 in Patients Discharged From Hospital - A Cohort StudyDocument14 pages!6-Month Consequences of COVID-19 in Patients Discharged From Hospital - A Cohort StudyCARLA CRISTINA DE ARAUJONo ratings yet
- Journal Pone 0254580Document10 pagesJournal Pone 0254580tifanny carolinaNo ratings yet
- Development and Validation of A Preoperative Scoring System To Predict 30 Day Mortality in Patients Undergoing Hip Fracture SurgeryDocument7 pagesDevelopment and Validation of A Preoperative Scoring System To Predict 30 Day Mortality in Patients Undergoing Hip Fracture Surgeryuhs888No ratings yet
- Jamal 2014Document7 pagesJamal 2014Andi EsSeNo ratings yet
- Clinica Chimica Acta: SciencedirectDocument5 pagesClinica Chimica Acta: SciencedirectMauricioNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- Principales Emergencias Oncológicas en El Cáncer de Pulmón: Un Análisis de Un Único CentroDocument3 pagesPrincipales Emergencias Oncológicas en El Cáncer de Pulmón: Un Análisis de Un Único CentroJoskarla MontillaNo ratings yet
- Procalcitonina ITUDocument7 pagesProcalcitonina ITUJohana Zamudio RojasNo ratings yet
- Journal SepsisDocument8 pagesJournal Sepsisarif21492No ratings yet
- 2015 BJMMR 18180rev1Document14 pages2015 BJMMR 18180rev1Hülya SungurtekinNo ratings yet
- Crit Care - Acute Abdominal Pain - Gajic (2002) Acute Abdomen in Mthe Medical Intensive Care UnitDocument4 pagesCrit Care - Acute Abdominal Pain - Gajic (2002) Acute Abdomen in Mthe Medical Intensive Care UnitjNo ratings yet
- Predictive Biomarkers For Complicated Acute Appendicitis 2020Document9 pagesPredictive Biomarkers For Complicated Acute Appendicitis 2020Ricardo Javier Arreola PeraltaNo ratings yet
- Antibiotic Timing Sepsis MortalityDocument15 pagesAntibiotic Timing Sepsis MortalityRichard BunNo ratings yet
- Classifying Patients Suspected of Appendicitis With Regard To LikelihoodDocument6 pagesClassifying Patients Suspected of Appendicitis With Regard To LikelihoodabybmusNo ratings yet
- Pan 23Document11 pagesPan 23Asad KakarNo ratings yet
- Fallo Renal en COVID19Document11 pagesFallo Renal en COVID19Kristel SalvatierraNo ratings yet
- Admin A 10 1 85 3b9f306Document8 pagesAdmin A 10 1 85 3b9f306Dyanne BautistaNo ratings yet
- Quick Sepsis-Related OrganDocument12 pagesQuick Sepsis-Related OrganArnavjyoti DasNo ratings yet
- Apache 3Document10 pagesApache 3Priyadarshan NairNo ratings yet
- Predicting Mortality and Morbidity of Patients Operated On For Perforated Peptic UlcersDocument5 pagesPredicting Mortality and Morbidity of Patients Operated On For Perforated Peptic UlcersbintixxNo ratings yet
- S014067362305663 PDFDocument9 pagesS014067362305663 PDFfenixNo ratings yet
- Blood Urea Nitrogen in The Early Assessment of Acute PancreatitisDocument8 pagesBlood Urea Nitrogen in The Early Assessment of Acute PancreatitisRicardo Uzcategui ArreguiNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Fagon, Bronch Vs Clinical DX VAP. Annals Int Med. 2000Document10 pagesFagon, Bronch Vs Clinical DX VAP. Annals Int Med. 2000Abhishek GoelNo ratings yet
- jgh3 12342Document10 pagesjgh3 1234221amrikamaharajNo ratings yet
- Renal and Perinephric Abscesses: Analysis of 65 Consecutive CasesDocument6 pagesRenal and Perinephric Abscesses: Analysis of 65 Consecutive CasesGio Eleceene LyneyNo ratings yet
- PMK No. 43 TTG Penyelenggaraan Laboratorium Klinik Yang BaikDocument16 pagesPMK No. 43 TTG Penyelenggaraan Laboratorium Klinik Yang BaikyantuNo ratings yet
- Covid19 - Consecuencias A 6 MesesDocument13 pagesCovid19 - Consecuencias A 6 MesesSMIBA MedicinaNo ratings yet
- Adamik B Et Al. Arch Immunol. 2015Document9 pagesAdamik B Et Al. Arch Immunol. 2015goutham sivasailamNo ratings yet
- Supplementary Table (Data Underlying) :: Mysticeti (Baleen Whales)Document27 pagesSupplementary Table (Data Underlying) :: Mysticeti (Baleen Whales)rppawar_321203003No ratings yet
- Brief NP Vs P Explain2Document8 pagesBrief NP Vs P Explain2rppawar_321203003No ratings yet
- Brief NP Vs P Explain2Document8 pagesBrief NP Vs P Explain2rppawar_321203003No ratings yet
- Fig S2Document1 pageFig S2rppawar_321203003No ratings yet
- Wild-Type: Transformant Nmat2 Plants Nmat2Document1 pageWild-Type: Transformant Nmat2 Plants Nmat2rppawar_321203003No ratings yet
- Mccollough Effect: A Neural Network Model Based On Source SeparationDocument19 pagesMccollough Effect: A Neural Network Model Based On Source Separationrppawar_321203003No ratings yet
- Supporting Information: Experimental Details 1. Preparation of Langmuir-Blodgett FilmsDocument14 pagesSupporting Information: Experimental Details 1. Preparation of Langmuir-Blodgett Filmsrppawar_321203003No ratings yet
- Journal of Petroleum Science and EngineeringDocument24 pagesJournal of Petroleum Science and Engineeringrppawar_321203003No ratings yet
- Ripple: Overview and Outlook: August 2015Document19 pagesRipple: Overview and Outlook: August 2015rppawar_321203003No ratings yet
- Supplementary Materials: Track 1 - Ascending, Binary, LowDocument6 pagesSupplementary Materials: Track 1 - Ascending, Binary, Lowrppawar_321203003No ratings yet
- Three Weeks of Autoregulation Training Increases The Load-Velocity, - RPE and - RIR Relationships in Experienced AthletesDocument14 pagesThree Weeks of Autoregulation Training Increases The Load-Velocity, - RPE and - RIR Relationships in Experienced Athletesrppawar_321203003No ratings yet
- Es0c06789 Si 001Document28 pagesEs0c06789 Si 001rppawar_321203003No ratings yet
- Astractdetails 0000656770Document2 pagesAstractdetails 0000656770rppawar_321203003No ratings yet
- Supplementary Materials For Tjoe-2020-0036Document13 pagesSupplementary Materials For Tjoe-2020-0036rppawar_321203003No ratings yet
- Elsevier Trypolska 2019Document9 pagesElsevier Trypolska 2019rppawar_321203003No ratings yet
- Probability Density FunctionDocument19 pagesProbability Density Functionrppawar_321203003No ratings yet
- Appendix 1Document8 pagesAppendix 1rppawar_321203003No ratings yet
- Two General Schemes of Algebraic Cryptography: Groups October 2018Document17 pagesTwo General Schemes of Algebraic Cryptography: Groups October 2018rppawar_321203003No ratings yet
- 2016 Crip To Currency I JB MCDocument10 pages2016 Crip To Currency I JB MCAnonymous 5dzNTLcergNo ratings yet
- Free Research ReportsDocument205 pagesFree Research ReportsRajkumar TiwariNo ratings yet
- SRFresearchReportFINAL2013 PDFDocument28 pagesSRFresearchReportFINAL2013 PDFmikalraNo ratings yet
- Cryptocurrency Article PDFDocument11 pagesCryptocurrency Article PDFAnkurNo ratings yet
- SRFresearchReportFINAL2013 PDFDocument28 pagesSRFresearchReportFINAL2013 PDFmikalraNo ratings yet
- Research Report SamplesDocument87 pagesResearch Report Samplesrppawar_321203003No ratings yet
- Undergraduate Research Reports Update 051112 PDFDocument2 pagesUndergraduate Research Reports Update 051112 PDFAdam Bin Mat RofiNo ratings yet
- Research Report Examples PDFDocument170 pagesResearch Report Examples PDFMaithili SUBRAMANIANNo ratings yet
- Writing Research Report: July 2016Document22 pagesWriting Research Report: July 2016Md. Faruq HasanNo ratings yet
- Sample Research ReportDocument15 pagesSample Research Reportrppawar_321203003No ratings yet
- Research Report PDFsDocument47 pagesResearch Report PDFsrppawar_321203003No ratings yet
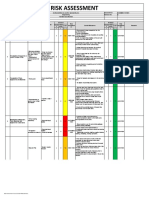
- ICS SMNCI RA 001 Temfacil ConstructionDocument7 pagesICS SMNCI RA 001 Temfacil ConstructionJayson Escamillan100% (1)
- 2 Story Telling Templetes 2023Document1 page2 Story Telling Templetes 2023serkovanastya12No ratings yet
- Introduction To Automation: BITS PilaniDocument25 pagesIntroduction To Automation: BITS PilaniymsyaseenNo ratings yet
- Brunei Shell EOI QualificationsDocument40 pagesBrunei Shell EOI QualificationsSyed Abdul RahmanNo ratings yet
- IUCAA ReportDocument4 pagesIUCAA ReportRADHIKA BHARADIYANo ratings yet
- Factoring Using Common Monomial FactorDocument26 pagesFactoring Using Common Monomial FactorHappyNo ratings yet
- LAC Reflection JournalDocument6 pagesLAC Reflection JournalEDITHA QUITO100% (1)
- Dhyg 415 Study Guide Yezi Pang - 1Document117 pagesDhyg 415 Study Guide Yezi Pang - 1api-473128642No ratings yet
- MSC 2011-10S370Document70 pagesMSC 2011-10S370caraiane100% (2)
- Lec29 PDFDocument32 pagesLec29 PDFVignesh Raja PNo ratings yet
- CarringtonDocument29 pagesCarringtonTaryn Lee AverittNo ratings yet
- Lesson 1 - Environmental PrinciplesDocument26 pagesLesson 1 - Environmental PrinciplesGeroline SaycoNo ratings yet
- Available at VTU HUB (Android App) : Atme College of Engineering, MysuruDocument32 pagesAvailable at VTU HUB (Android App) : Atme College of Engineering, MysuruRahul Singh PariharNo ratings yet
- Synetek Controls Inc.: Ds1-S: Installation InstructionsDocument2 pagesSynetek Controls Inc.: Ds1-S: Installation Instructionsdgd_electromecNo ratings yet
- Ecofeminism in Amazonian EcuadorDocument28 pagesEcofeminism in Amazonian EcuadorAnna Carolina Fornero AguiarNo ratings yet
- Ce121 Lec5 BuoyancyDocument18 pagesCe121 Lec5 BuoyancyPetForest Ni JohannNo ratings yet
- Say It With Charts - McKinsey-32Document4 pagesSay It With Charts - McKinsey-32YONGXING CHENNo ratings yet
- Session 4 Stephanie CicchiniDocument20 pagesSession 4 Stephanie CicchiniMarinos GounaridisNo ratings yet
- Ball Mill Dynamics: GRINDING I - Training SessionDocument45 pagesBall Mill Dynamics: GRINDING I - Training SessionFran jimenezNo ratings yet
- Response of Buried Pipes Taking Into Account Seismic and Soil Spatial VariabilitiesDocument8 pagesResponse of Buried Pipes Taking Into Account Seismic and Soil Spatial VariabilitiesBeh RangNo ratings yet
- OralCom q1 Mod3 Barrierstocommunciation v5Document33 pagesOralCom q1 Mod3 Barrierstocommunciation v5KryssssNo ratings yet
- DLP-Compound Sentences To Show Cause and Effect RelationshipDocument1 pageDLP-Compound Sentences To Show Cause and Effect RelationshipJocelyn G. EmpinadoNo ratings yet
- Article Nejib SeismoDocument25 pagesArticle Nejib SeismoseimedNo ratings yet
- CPM Precalculus Homework AnswersDocument7 pagesCPM Precalculus Homework Answerscqxxvzhlf100% (1)
- Institute For Career Research Editors - Careers in Medical Research-Institute For Career Research (2007)Document32 pagesInstitute For Career Research Editors - Careers in Medical Research-Institute For Career Research (2007)Cynthia CNo ratings yet
- Chapter4-Working With Dask Bags For Unstructured DataDocument33 pagesChapter4-Working With Dask Bags For Unstructured DataKomi David ABOTSITSENo ratings yet
- BSCE Worksheet Mod 3 Lessons12 - FAMILY-NAME-3Document7 pagesBSCE Worksheet Mod 3 Lessons12 - FAMILY-NAME-3RINCONADA ReynalynNo ratings yet
- Norma Iso 5630-Parte 3Document12 pagesNorma Iso 5630-Parte 3Nestor Mejia LondoñoNo ratings yet
- ObjectScript ReferenceDocument4 pagesObjectScript ReferenceRodolfoNo ratings yet
- TimelineDocument2 pagesTimelineapi-240600220No ratings yet