You might also like
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- Board Certified Nurse Practitioner in Savannah GA Resume Michele StephensDocument4 pagesBoard Certified Nurse Practitioner in Savannah GA Resume Michele StephensMicheleStephens100% (1)
- Intern Survival Guide The UNC Department of MedicineDocument22 pagesIntern Survival Guide The UNC Department of MedicinecmirceaNo ratings yet
- The Intern Pocket Card Surviving GraysDocument2 pagesThe Intern Pocket Card Surviving GraysKathleen Grace ManiagoNo ratings yet
- Referral Cheat Sheet: Before You CallDocument2 pagesReferral Cheat Sheet: Before You CallXyz100% (2)
- House MD Notes Handbook PrototypeDocument78 pagesHouse MD Notes Handbook PrototypeBea Samonte100% (2)
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- Care Plan Handbook TemplateDocument34 pagesCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Cardiology Step 2 CK NotesDocument5 pagesCardiology Step 2 CK NotesVidur S SinghNo ratings yet
- CC and MCC List For DRG CodingDocument1 pageCC and MCC List For DRG Codinge-MedTools100% (2)
- Clinical Examinations Crib Sheet v7Document36 pagesClinical Examinations Crib Sheet v7aparish10100% (1)
- Hypertension Follow Up EvaluationDocument1 pageHypertension Follow Up Evaluatione-MedTools100% (3)
- Electronic Medical TextbooksDocument4 pagesElectronic Medical TextbooksProf Rakesh Sharma80% (5)
- A. Subjective: 1. Progress NoteDocument3 pagesA. Subjective: 1. Progress NoteEvan100% (1)
- Eclinicalworks Clinician Training Guide: OutlineDocument40 pagesEclinicalworks Clinician Training Guide: OutlineStephany GrandersonNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- Top 200 Drug Study Reference RLPDocument31 pagesTop 200 Drug Study Reference RLPYathrika YathrikaNo ratings yet
- Clinical Handover Ian ScottDocument26 pagesClinical Handover Ian ScottYwagar YwagarNo ratings yet
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- SHOCK Slide WorkbookDocument10 pagesSHOCK Slide WorkbookPATHMAPRIYA GANESANNo ratings yet
- Know The Normal ValuesDocument3 pagesKnow The Normal ValuesAngeline Monilla PanteNo ratings yet
- Intern Survival Guide 2014-2015Document145 pagesIntern Survival Guide 2014-2015Katie Kroll BradyNo ratings yet
- Case PresentationDocument30 pagesCase PresentationAmira HelayelNo ratings yet
- Notes For Clincal CasesDocument12 pagesNotes For Clincal CasesMandeepNo ratings yet
- 3639 - Basic Patient DataDocument1 page3639 - Basic Patient DataRaven247No ratings yet
- ABG Interpretation - ATSDocument5 pagesABG Interpretation - ATSHAMMYER ALROKHAMINo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- SOAP Note TemplateDocument1 pageSOAP Note Templatenmb1986No ratings yet
- Clinicalmedicine Notes OsceDocument18 pagesClinicalmedicine Notes OsceSindu Sai0% (1)
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- IV Solution Cheat Sheet: A Quick Reference Guide On The Different Intravenous SolutionsDocument2 pagesIV Solution Cheat Sheet: A Quick Reference Guide On The Different Intravenous SolutionsMehdi SabeiNo ratings yet
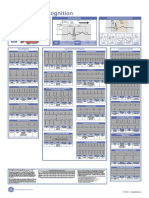
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- Atrial Fibrillation Topic DiscussionDocument23 pagesAtrial Fibrillation Topic Discussionapi-567600964No ratings yet
- PCM Guidebook For History Taking and Physical Exam, Revised Final, 9-20-17Document82 pagesPCM Guidebook For History Taking and Physical Exam, Revised Final, 9-20-17anon_925247980No ratings yet
- Weekly Clinical Prep Packet 12 REVISEDDocument12 pagesWeekly Clinical Prep Packet 12 REVISEDMei SarteNo ratings yet
- Vitamin Chart 2Document3 pagesVitamin Chart 2surviving nursing schoolNo ratings yet
- Index: NURS 2236 Clinical Form 3: Clinical Medications WorksheetDocument2 pagesIndex: NURS 2236 Clinical Form 3: Clinical Medications WorksheetEthel NormanNo ratings yet
- PD OSCE GuideDocument19 pagesPD OSCE GuideChorong ParkNo ratings yet
- ABG InterpretationDocument11 pagesABG InterpretationertrggerNo ratings yet
- Medgeeks: Pharmacology Cheat SheetsDocument13 pagesMedgeeks: Pharmacology Cheat SheetsJuan Jose CastroNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Patient Information FormDocument6 pagesPatient Information FormKimCriglerNo ratings yet
- Powerchart Review Guide v2 1rpDocument6 pagesPowerchart Review Guide v2 1rpapi-224958119No ratings yet
- Electrolyte Mnemonic QuizletDocument3 pagesElectrolyte Mnemonic QuizletA.h.Murad100% (2)
- Sbar 3Document1 pageSbar 3Nurse Betty100% (1)
- Aprn PresentationDocument12 pagesAprn Presentationapi-234511817No ratings yet
- Internal Med TipsDocument2 pagesInternal Med TipsNick100% (1)
- Diabetes Insulin Oral Agents TreatmentDocument1 pageDiabetes Insulin Oral Agents TreatmentAudrey Nicole GabianaNo ratings yet
- Arrythmia Name: Normal Sinus RhythmDocument7 pagesArrythmia Name: Normal Sinus RhythmJulx0No ratings yet
- Antibiotics Chart 1Document7 pagesAntibiotics Chart 1Vee MendNo ratings yet
- SBAR TemplateDocument1 pageSBAR TemplateBella SmithNo ratings yet
- Common Medical NotationsDocument3 pagesCommon Medical NotationssaltarisNo ratings yet
- HistoryandPhysicalExamDocument105 pagesHistoryandPhysicalExamsilentscream0618No ratings yet
- Clinical Guidelines and Care ProtocolsFrom EverandClinical Guidelines and Care ProtocolsRating: 5 out of 5 stars5/5 (1)
- Pediatric Cardiology and Pulmonology: A Practically Painless ReviewFrom EverandPediatric Cardiology and Pulmonology: A Practically Painless ReviewNo ratings yet
- Addiction in the Lives of Registered Nurses and Their Wake-Up Jolt to RecoveryFrom EverandAddiction in the Lives of Registered Nurses and Their Wake-Up Jolt to RecoveryNo ratings yet
- Certified Laboratory Assistant: Passbooks Study GuideFrom EverandCertified Laboratory Assistant: Passbooks Study GuideNo ratings yet
- Guideline - Obs & GynDocument194 pagesGuideline - Obs & GynGood MaishaNo ratings yet
- KiAmins SurgeryDocument211 pagesKiAmins SurgeryGood MaishaNo ratings yet
- An Introduction To The World Health OrganisationDocument26 pagesAn Introduction To The World Health Organisationapi-253150011No ratings yet
- s6.2 - Surgical Antibiotic ProphylaxisDocument28 pagess6.2 - Surgical Antibiotic ProphylaxisvladinhoNo ratings yet
- Overnight Events Interdisciplinary Notes Vital Signs I/O and WeightsDocument8 pagesOvernight Events Interdisciplinary Notes Vital Signs I/O and WeightsGood MaishaNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- Arterial Blood Gas (ABG) Analysis: Normal ValuesDocument3 pagesArterial Blood Gas (ABG) Analysis: Normal ValuesNayem Hossain HemuNo ratings yet
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Knowledge Regarding Prevention of Helminthic Disease Among School ChildrenDocument5 pagesKnowledge Regarding Prevention of Helminthic Disease Among School ChildrenIJAR JOURNALNo ratings yet
- Tn-I Plus: Warnings and PrecautionsDocument5 pagesTn-I Plus: Warnings and PrecautionsAniket DubeyNo ratings yet
- Case Study (Aub)Document16 pagesCase Study (Aub)Lucila Lugo0% (2)
- Introduction To Physical ExaminationDocument13 pagesIntroduction To Physical ExaminationMuhammad SyarmineNo ratings yet
- Hemolytic Disease of The NewbornDocument16 pagesHemolytic Disease of The NewbornStanculescu MarianaNo ratings yet
- Introduction To PathologyDocument40 pagesIntroduction To PathologyJugun HayatNo ratings yet
- Estudio Ácido UndecilenicoDocument3 pagesEstudio Ácido UndecilenicocarbouNo ratings yet
- History Taking and Examination For SurgeryDocument68 pagesHistory Taking and Examination For Surgerytayiba.m1995No ratings yet
- Advocacy in PharmacyDocument3 pagesAdvocacy in PharmacyZofia RanadaNo ratings yet
- Hemant Surgical Double Lumen CathetersDocument2 pagesHemant Surgical Double Lumen CathetersKaushik Hanskumar ShahNo ratings yet
- 120 HAAD Exam QuestionsDocument10 pages120 HAAD Exam QuestionsConsolacion Binarao Dolores50% (8)
- QUIZ No. 3 Questions 150 ItemsDocument14 pagesQUIZ No. 3 Questions 150 ItemsxaileenxNo ratings yet
- Pain Management in AnimalsDocument184 pagesPain Management in Animalsssarbovan100% (1)
- General Post Operative Nursing Care of A PatientDocument55 pagesGeneral Post Operative Nursing Care of A PatientFan Eli100% (2)
- 2020 Article 2297 PDFDocument11 pages2020 Article 2297 PDFPamela Alejandra Marín VillalónNo ratings yet
- Causes of Upper Gastrointestinal Bleeding in Adults UpToDateDocument37 pagesCauses of Upper Gastrointestinal Bleeding in Adults UpToDateJodene Rose RojasNo ratings yet
- Anaesthesia For Trauma PatientsDocument42 pagesAnaesthesia For Trauma PatientsMerindukan Surga MuNo ratings yet
- Dissertation On Cancer ResearchDocument5 pagesDissertation On Cancer ResearchWhereToBuyWritingPaperUK100% (1)
- Resume Anna BalancioDocument3 pagesResume Anna Balanciojihn isis tengcoNo ratings yet
- Dengue Presentation (KEMU)Document90 pagesDengue Presentation (KEMU)MuhammadTalhaNo ratings yet
- Health Consideration at Work Place: Airborne DiseasesDocument12 pagesHealth Consideration at Work Place: Airborne DiseasesvishwaNo ratings yet
- Guidance To The Internaitonal Medical Guide For Ships 3rd EdDocument14 pagesGuidance To The Internaitonal Medical Guide For Ships 3rd EdSaurabh YadavNo ratings yet
- Name - Alafia AzharDocument5 pagesName - Alafia AzharZafir AnsariNo ratings yet
- Anti HAVDocument3 pagesAnti HAVHassan GillNo ratings yet
- Diseases of ImmunityDocument13 pagesDiseases of ImmunityRose AnnNo ratings yet
- Risk For Infection Related To High Glucose LevelsDocument2 pagesRisk For Infection Related To High Glucose LevelsDanica Kate GalleonNo ratings yet
- Vocabulary Work Book Check Your English Vocabulary For MedicineDocument50 pagesVocabulary Work Book Check Your English Vocabulary For MedicineMarius Belean100% (1)
- Lesson Plan Reproductive SystemDocument3 pagesLesson Plan Reproductive SystemMaryJoyceReyes50% (2)