You might also like
- Oh No, It's A Big Fat Bitch SpayDocument8 pagesOh No, It's A Big Fat Bitch SpayWilliam Chandler100% (1)
- Group 3 Cardiovascular ProblemDocument52 pagesGroup 3 Cardiovascular ProblemWARREN WILLIAM PERAN100% (3)
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
- Surgery Okell Notes 2Document205 pagesSurgery Okell Notes 2Youzuf Iqbal100% (1)
- TEACHING PLAN FOR Varicose VeinsDocument5 pagesTEACHING PLAN FOR Varicose Veinscertified_maharot_ako2828No ratings yet
- Kelenjar BartoliniDocument15 pagesKelenjar BartolinionlyfellaNo ratings yet
- Kelenjar BartoliniDocument15 pagesKelenjar BartolinionlyfellaNo ratings yet
- Bartholin's Gland Cysts/Abscesses: Causes, Symptoms and Surgical TreatmentsDocument6 pagesBartholin's Gland Cysts/Abscesses: Causes, Symptoms and Surgical TreatmentsJane NathaniaNo ratings yet
- XXXXDocument27 pagesXXXXIlham HarsyaNo ratings yet
- Pap Smear & Diagnostic Tests for Female Reproductive OrgansDocument13 pagesPap Smear & Diagnostic Tests for Female Reproductive Organsta CNo ratings yet
- Clinical Pathology of Bartholin's Glands ReviewDocument14 pagesClinical Pathology of Bartholin's Glands ReviewNorman AjxNo ratings yet
- Bartholin Gland DuctDocument2 pagesBartholin Gland DuctJustin Ahorro-DionisioNo ratings yet
- Vulvar Abscess Guide: Causes, Symptoms and TreatmentDocument5 pagesVulvar Abscess Guide: Causes, Symptoms and TreatmentsalamredNo ratings yet
- Kista BartoliniDocument24 pagesKista BartoliniTri HariadyNo ratings yet
- Bartholin's Gland ExcisionDocument4 pagesBartholin's Gland ExcisionIndra JayaNo ratings yet
- BARTHOLIN GLAND DISEASESDocument13 pagesBARTHOLIN GLAND DISEASESgabriella azaliaNo ratings yet
- Benign Neoplasms of the Vulva, Vagina, Cervix and UterusDocument11 pagesBenign Neoplasms of the Vulva, Vagina, Cervix and UterusIrene FranzNo ratings yet
- Clinical Case Analysis Ectopic PregnancyDocument4 pagesClinical Case Analysis Ectopic PregnancySiobhan GreeneNo ratings yet
- Scrotal AbnormalitiesDocument6 pagesScrotal AbnormalitiesmoominjunaidNo ratings yet
- SherylDocument2 pagesSherylRio C. PangahasNo ratings yet
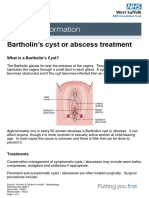
- Bartholin's Cyst or Abscess TreatmentDocument4 pagesBartholin's Cyst or Abscess TreatmentRezaFArthaNo ratings yet
- Incision and Drainage of Scrotal AbscessDocument31 pagesIncision and Drainage of Scrotal AbscessRm LavariasNo ratings yet
- Midwifery - SterlizationDocument39 pagesMidwifery - SterlizationEsha KuttiNo ratings yet
- Cervicalpolyp 12345Document14 pagesCervicalpolyp 12345faikaoesmaniaNo ratings yet
- Scrotal Swelling2Document26 pagesScrotal Swelling2bigtemptationNo ratings yet
- د.معد Tumers of Vagina-2 (Muhadharaty)Document25 pagesد.معد Tumers of Vagina-2 (Muhadharaty)Ali EmadNo ratings yet
- Understanding Common Causes of Scrotal SwellingsDocument35 pagesUnderstanding Common Causes of Scrotal SwellingsYohanna SinuhajiNo ratings yet
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- Fistula PerianalDocument25 pagesFistula PerianalHafiizh Dwi PramuditoNo ratings yet
- Breast Diseases GuideDocument53 pagesBreast Diseases GuideAbdullah EssaNo ratings yet
- Genital FistulaeDocument15 pagesGenital Fistulaesangeetha francisNo ratings yet
- Scrotal Swelling FadhlyDocument52 pagesScrotal Swelling FadhlyfadhlyNo ratings yet
- Anal and Perianal ConditionsDocument58 pagesAnal and Perianal ConditionsYonas YemidiralemNo ratings yet
- Scrotal SwellingDocument40 pagesScrotal Swellingeirene simbolonNo ratings yet
- Abdominal X-Rays PT 1Document20 pagesAbdominal X-Rays PT 1sb medexNo ratings yet
- Abnormalities in Vagina and VulvaDocument32 pagesAbnormalities in Vagina and VulvaNovia RizqiNo ratings yet
- Male Genital Organs Clinical Marija DjuricDocument31 pagesMale Genital Organs Clinical Marija DjuricНемосјановић ЋудмилаNo ratings yet
- 25 UrologyDocument47 pages25 UrologyMahmoud AbuAwadNo ratings yet
- Bladder CancerDocument3 pagesBladder CancerGhea Jovita SinagaNo ratings yet
- Genito-Urinary Fistulas: Yashar Najiaghdam M.DDocument33 pagesGenito-Urinary Fistulas: Yashar Najiaghdam M.DRahul ChopadeNo ratings yet
- Speculum ExaminationDocument3 pagesSpeculum ExaminationShum Wing Hei JoanneNo ratings yet
- Understanding Hydroceles: Causes, Symptoms and TreatmentDocument39 pagesUnderstanding Hydroceles: Causes, Symptoms and TreatmentNd Eye100% (2)
- Reproductive - Genital System-2Document26 pagesReproductive - Genital System-2Muhammad Faheem AslamNo ratings yet
- Infant Umbilical AbnormalitiesDocument59 pagesInfant Umbilical AbnormalitieskedokterankeluargaNo ratings yet
- Scrotal MassesDocument19 pagesScrotal MassesJohnNo ratings yet
- Dr. Trika-Pit Hugi TIDocument37 pagesDr. Trika-Pit Hugi TIMunifah YusriyahNo ratings yet
- Varicocele Guide: Causes, Diagnosis & TreatmentDocument65 pagesVaricocele Guide: Causes, Diagnosis & TreatmentParamartha KesumaNo ratings yet
- UntitledDocument60 pagesUntitledVenkatapradeepNo ratings yet
- Cervical Polyp 12345Document13 pagesCervical Polyp 12345Osama Edris Hama SamanNo ratings yet
- BreastDocument8 pagesBreastNada MuchNo ratings yet
- Surgery NotesDocument127 pagesSurgery NotesDawit KimNo ratings yet
- Pathophysiology: Each Month, Normally Functioning Ovaries Develop SmallDocument9 pagesPathophysiology: Each Month, Normally Functioning Ovaries Develop SmallAl-nazer Azer Al100% (1)
- Testicular Torsion, Hydrocele & Fournier GangreneDocument41 pagesTesticular Torsion, Hydrocele & Fournier GangreneNur Insyirah100% (1)
- Genitourinary Fistulas: Causes, Types, Diagnosis and ManagementDocument33 pagesGenitourinary Fistulas: Causes, Types, Diagnosis and ManagementDzulRizkaNo ratings yet
- Ejgm 166Document3 pagesEjgm 166Melissa ArinieNo ratings yet
- Colposcopy ExaminationDocument15 pagesColposcopy Examinationsapana shahNo ratings yet
- Varicocele and Eo l2Document8 pagesVaricocele and Eo l2youssef.aziz2020No ratings yet
- Pediatric EmergencyDocument66 pagesPediatric EmergencyWaseem MoukhtarNo ratings yet
- Genito-Urinary FistulaDocument33 pagesGenito-Urinary Fistuladr_asaleh100% (4)
- URINARY SYSTEMDocument18 pagesURINARY SYSTEMAbdusaburNo ratings yet
- Introduction to Breast Diseases and Nipple DischargesDocument10 pagesIntroduction to Breast Diseases and Nipple DischargessintayehuNo ratings yet
- Genito-Urinary Fistulas: Yashar Najiaghdam M.DDocument33 pagesGenito-Urinary Fistulas: Yashar Najiaghdam M.DyoghaNo ratings yet
- MSU GS PolicyDocument42 pagesMSU GS PolicyElvisNo ratings yet
- STANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaDocument40 pagesSTANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaElvisNo ratings yet
- Hypertension in Adults Diagnosis and Management PDF 66141722710213Document47 pagesHypertension in Adults Diagnosis and Management PDF 66141722710213ElvisNo ratings yet
- National Guidelines For Safe Management of Health Care Waste Final1Document82 pagesNational Guidelines For Safe Management of Health Care Waste Final1ElvisNo ratings yet
- Pediatric Medical Emergencies Rev Oct 2016Document27 pagesPediatric Medical Emergencies Rev Oct 2016ElvisNo ratings yet
- Harrison Notes Demo Medicalsupernotes PDFDocument50 pagesHarrison Notes Demo Medicalsupernotes PDFmikeNo ratings yet
- Asthma GuideDocument2 pagesAsthma GuideJearome TaboyNo ratings yet
- Pre-internship questions on medical topicsDocument8 pagesPre-internship questions on medical topicsPeprah OndibaNo ratings yet
- How To Write A Research ProposalDocument5 pagesHow To Write A Research Proposalhuwaina100% (1)
- General Surgery A Revision Session For FinalsDocument69 pagesGeneral Surgery A Revision Session For Finalsimperiallight100% (1)
- Dysentery (S) : C WHO G WHO E M LDocument33 pagesDysentery (S) : C WHO G WHO E M LgregoryNo ratings yet
- Biology Volunteer Instructions 11-30-16Document7 pagesBiology Volunteer Instructions 11-30-16ElvisNo ratings yet
- 231 Biology F2Document1 page231 Biology F2ElvisNo ratings yet
- Transcript2021feb05 DCM 2017 71788Document5 pagesTranscript2021feb05 DCM 2017 71788ElvisNo ratings yet
- Review of SystemsDocument1 pageReview of SystemsZuellen Mae Garapan BedañoNo ratings yet
- Management of Postpartum Haemorrhage (C Obs 43) Review July 2017Document17 pagesManagement of Postpartum Haemorrhage (C Obs 43) Review July 2017ElvisNo ratings yet
- Standard Treatment GuidelinesDocument431 pagesStandard Treatment Guidelinesadnan khanNo ratings yet
- Puerperium and Its Management 1Document35 pagesPuerperium and Its Management 1Elvis100% (2)
- Problems in Early Pregnancy - NBT002073Document8 pagesProblems in Early Pregnancy - NBT002073ElvisNo ratings yet
- Pediatrics National Clinical Treatment Guideline Ok Version After CorrectionsDocument176 pagesPediatrics National Clinical Treatment Guideline Ok Version After CorrectionsmomocamuiNo ratings yet
- Burns Definition Classification Pathophysiology and Initial Approach 2327 5146 1000298Document5 pagesBurns Definition Classification Pathophysiology and Initial Approach 2327 5146 1000298Alexandra Ançã PiresNo ratings yet
- BoneDocument8 pagesBoneElvisNo ratings yet
- Juvenile ArthritisDocument11 pagesJuvenile ArthritisElvisNo ratings yet
- 31 - Early Pregnancy Bleeding-1Document8 pages31 - Early Pregnancy Bleeding-1ElvisNo ratings yet
- Online CPD: Monitoring Labour Using A PartographDocument28 pagesOnline CPD: Monitoring Labour Using A PartographElvisNo ratings yet
- Relieve Back Pain with Protruded Disc TreatmentDocument12 pagesRelieve Back Pain with Protruded Disc TreatmentElvisNo ratings yet
- Cerebrovascular Accident/Brain Attack: Gideon Gachihi Associate Faculty, MKUDocument52 pagesCerebrovascular Accident/Brain Attack: Gideon Gachihi Associate Faculty, MKUElvisNo ratings yet
- The Physiology of The SkinDocument39 pagesThe Physiology of The SkinElvisNo ratings yet
- Dermatology Updated 2020Document57 pagesDermatology Updated 2020ElvisNo ratings yet
- Invasive Cervical Traction Gardner Wells TongsDocument3 pagesInvasive Cervical Traction Gardner Wells TongsErvan Hartanto ErvanNo ratings yet
- Structures and Functions of Living OrganismsDocument28 pagesStructures and Functions of Living OrganismsMarianna HernandezNo ratings yet
- Must To Know in Immunohematology (Blood Banking)Document25 pagesMust To Know in Immunohematology (Blood Banking)Tokita OhmaNo ratings yet
- Developmental History Form 2016Document5 pagesDevelopmental History Form 2016Mariya KhanNo ratings yet
- Descriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamDocument5 pagesDescriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamAditya HendraNo ratings yet
- Koenig Pastoral Counseling With The AgedDocument11 pagesKoenig Pastoral Counseling With The AgedDavid Danao Franco MendezNo ratings yet
- Random Blood Sugar Test AssignmentDocument1 pageRandom Blood Sugar Test AssignmentmadamcloudnineNo ratings yet
- UM-DP12-25R UM-DP20-25R: The World's First Ultrasonic Probes With Dual-Plane Reconstruction Scanning CapabilityDocument3 pagesUM-DP12-25R UM-DP20-25R: The World's First Ultrasonic Probes With Dual-Plane Reconstruction Scanning CapabilityRicardo PaterninaNo ratings yet
- Case Study: MargaretDocument2 pagesCase Study: MargaretmarielNo ratings yet
- Pain Medicine Board Review 1st EditionDocument52 pagesPain Medicine Board Review 1st Editionkevin.smart540No ratings yet
- Temporary Crown Care InstructionsDocument1 pageTemporary Crown Care InstructionsGhostOperativeNo ratings yet
- Common Asthma MedicationsDocument1 pageCommon Asthma MedicationsHeart of the Valley, Pediatric CardiologyNo ratings yet
- Risk Assessment Matrix (ISO) - 3Document1 pageRisk Assessment Matrix (ISO) - 3Verina GaldasNo ratings yet
- Simulation in Health Care Education: Perspectives in Biology and Medicine February 2008Document6 pagesSimulation in Health Care Education: Perspectives in Biology and Medicine February 2008Birendra MahatNo ratings yet
- Drugs and Substance AbuseDocument4 pagesDrugs and Substance Abusevaibhavch2904No ratings yet
- Anti-Obesity MedicationsDocument33 pagesAnti-Obesity MedicationsJorge Luis Alva AlonsoNo ratings yet
- VBMDocument24 pagesVBMSupervisor HCVNo ratings yet
- Hepatitis Case StudyDocument4 pagesHepatitis Case StudyTasha MageeNo ratings yet
- Potassium Chloride - Uses, Dosage & Side EffectsDocument4 pagesPotassium Chloride - Uses, Dosage & Side EffectsKenneth Mark B. TevesNo ratings yet
- Leann Li ResumeDocument2 pagesLeann Li Resumeapi-660140781No ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Mount Kenya UniversityDocument3 pagesMount Kenya UniversityAnonymous DGxdAOlNo ratings yet
- Current Clinical Strategies of Pancreatic CancerDocument28 pagesCurrent Clinical Strategies of Pancreatic CancerfikriafisNo ratings yet
- Cellular Regulation-BreastDocument41 pagesCellular Regulation-BreastMegan TurnerNo ratings yet
- HysterosDocument17 pagesHysterosAnto PopaNo ratings yet
- RisperidoneDocument3 pagesRisperidoneapi-3797941No ratings yet
- Headache Diagnosis and Treatment of 2609Document77 pagesHeadache Diagnosis and Treatment of 2609Reza Badruun Syahrul HakimNo ratings yet