You might also like
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- The Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentFrom EverandThe Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentRating: 4.5 out of 5 stars4.5/5 (3)
- N220 W8 Nursing Care Plan RevisedDocument3 pagesN220 W8 Nursing Care Plan RevisedVivian PhamNo ratings yet
- NCP - Acute Pain Related To EdemaDocument2 pagesNCP - Acute Pain Related To EdemaChenime Añana0% (1)
- Drug PercocetDocument1 pageDrug PercocetSrkocherNo ratings yet
- Nursing Care Plan: Non-Pharmacological Interventions: Distraction (TVDocument3 pagesNursing Care Plan: Non-Pharmacological Interventions: Distraction (TVVivian PhamNo ratings yet
- Care PlanDocument3 pagesCare Planbambam1aNo ratings yet
- Pain Management in Elderly Patients with Metastatic CancerDocument7 pagesPain Management in Elderly Patients with Metastatic CancerVALERIANO TRISHANo ratings yet
- Scenario:: Pain AssessmentDocument7 pagesScenario:: Pain AssessmentLouwella RamosNo ratings yet
- Regaining Mobility After Knee ReplacementDocument4 pagesRegaining Mobility After Knee ReplacementTameeka LockhartNo ratings yet
- MeperidineDocument3 pagesMeperidineGwyn RosalesNo ratings yet
- Subjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONDocument3 pagesSubjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONRona PieNo ratings yet
- PAIN management in adult AND GERIATRIC 2024 - CopyDocument58 pagesPAIN management in adult AND GERIATRIC 2024 - CopyclichegalNo ratings yet
- Drug Study Pre OpDocument6 pagesDrug Study Pre OpgiaNo ratings yet
- Assessment Nursing Diagnosis Planning Evaluation Objective of Care Intervention Rationale Subjective CuesDocument16 pagesAssessment Nursing Diagnosis Planning Evaluation Objective of Care Intervention Rationale Subjective CuesRoshin TejeroNo ratings yet
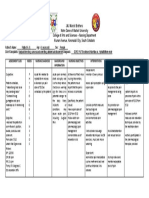
- JMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoDocument1 pageJMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoJoevence Gazo CuaresmaNo ratings yet
- NCPsDocument13 pagesNCPsdarwinNo ratings yet
- NSG Process JohnsonDocument11 pagesNSG Process JohnsonvishnukulakkadaNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanZyra AmbaganNo ratings yet
- Acute Gastroenteritis Case Study Nursing Care PlanDocument18 pagesAcute Gastroenteritis Case Study Nursing Care PlanKate Duque100% (1)
- Nursing Care Plan: Case ScenarioDocument14 pagesNursing Care Plan: Case ScenarioShelvin Jules LayvaNo ratings yet
- Subjective: Long Term: Independent:: Iloilo Doctors' College College of NursingDocument5 pagesSubjective: Long Term: Independent:: Iloilo Doctors' College College of NursingAbie Jean Balbontin100% (1)
- Chloe Jacoba NCMA 113 BSN 1-YC-6: Subjective IndependentDocument1 pageChloe Jacoba NCMA 113 BSN 1-YC-6: Subjective IndependentPatricia ParagguaNo ratings yet
- Nursing Care PlanDocument11 pagesNursing Care PlanJan DamesNo ratings yet
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesIvan Matthew SuperioNo ratings yet
- Senior Project ProductDocument7 pagesSenior Project Productapi-732018343No ratings yet
- Nursing Care ProcessDocument6 pagesNursing Care ProcessBerlyn FelicianoNo ratings yet
- Drug Study Case AnalysisDocument7 pagesDrug Study Case AnalysisNine SaguiboNo ratings yet
- Actual NCP Ortho - PESCADERO 4CDocument2 pagesActual NCP Ortho - PESCADERO 4COrlando VillanuevaNo ratings yet
- NCP Drug StudyDocument5 pagesNCP Drug StudyAndrea JoyaNo ratings yet
- 0orpilla Jomark C. Gerd - FdarDocument2 pages0orpilla Jomark C. Gerd - FdarAphrill Pearl PacisNo ratings yet
- Actual NCP - PESCADERO 4CDocument3 pagesActual NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- Nursing Care Plan (Acute Cholecystitis) - NAVARRADocument6 pagesNursing Care Plan (Acute Cholecystitis) - NAVARRAami forevsNo ratings yet
- Assessing and Managing Gastric PainDocument2 pagesAssessing and Managing Gastric PainMichael Joaquin0% (2)
- NCP For Pain (Appendicitis)Document2 pagesNCP For Pain (Appendicitis)Iris BalinoNo ratings yet
- Nurses Notes Date Focus Data Action Response: SubjectiveDocument2 pagesNurses Notes Date Focus Data Action Response: SubjectiveGILIANNE MARIE JIMENEANo ratings yet
- Palliative Care Management of ConstipationDocument5 pagesPalliative Care Management of ConstipationnehaNo ratings yet
- Nursing Care Plans for Pain & Pressure Ulcer ManagementDocument25 pagesNursing Care Plans for Pain & Pressure Ulcer ManagementZhyraine CaluzaNo ratings yet
- Department of Family and Community Medicine: Brokenshire Integrated Health Ministries Inc. Madapo Hills, Davao CityDocument13 pagesDepartment of Family and Community Medicine: Brokenshire Integrated Health Ministries Inc. Madapo Hills, Davao CityDonna Rose Gallera BobilaNo ratings yet
- NCP NewDocument16 pagesNCP Newmsfts.No ratings yet
- Concept Map FinalDocument1 pageConcept Map Finalapi-383763177No ratings yet
- ASSESSMENT OF ABDOMINAL PAIN AND NURSING INTERVENTIONSDocument4 pagesASSESSMENT OF ABDOMINAL PAIN AND NURSING INTERVENTIONSMikko McDonie VeloriaNo ratings yet
- NURSING CARE PLAN FOR APPENDICITISDocument7 pagesNURSING CARE PLAN FOR APPENDICITISHanz Abbigail Roco100% (1)
- Nursing Assessment Diagnosis GoalsDocument3 pagesNursing Assessment Diagnosis GoalsAngel HernandezNo ratings yet
- ActualDocument3 pagesActualSORIA CHOCNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanWinter SpringNo ratings yet
- Nursing Care Plan for Gallbladder StonesDocument3 pagesNursing Care Plan for Gallbladder StonesKristine YoungNo ratings yet
- 1N8 Abrio, Kyra Cheyenne NicholleDocument6 pages1N8 Abrio, Kyra Cheyenne NicholleKYRA CHEYENNE NICHOLLE ABRIONo ratings yet
- Patient Name: Maureen Wroble Age: 28 Years Old Gender: F C.S: Single BED#: #02 Date / Shift/ Time Focus Notes (Data, Action, Response)Document3 pagesPatient Name: Maureen Wroble Age: 28 Years Old Gender: F C.S: Single BED#: #02 Date / Shift/ Time Focus Notes (Data, Action, Response)mark OrpillaNo ratings yet
- NCM 116 SIDEnotes LeonorasDocument10 pagesNCM 116 SIDEnotes LeonorasChrizzha Mae Eredera EredianoNo ratings yet
- NCP PainDocument2 pagesNCP PainChristineAlaNo ratings yet
- NCP MedsurgeDocument2 pagesNCP MedsurgeGeddy SarigumbaNo ratings yet
- Nursing Care Plan UlcerDocument2 pagesNursing Care Plan Ulcerxrampley2100% (2)
- Breathing Problems Drowsiness, Dizziness Constipation, Nausea Vomiting Sweating Numbness, Tingling, or Cold Feeling in Your Hands and FeetDocument8 pagesBreathing Problems Drowsiness, Dizziness Constipation, Nausea Vomiting Sweating Numbness, Tingling, or Cold Feeling in Your Hands and FeetGino B. BulanaNo ratings yet
- Nursing Care Plan 3 Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan 3 Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationXena IngalNo ratings yet
- Assess Patient with Suspected AppendicitisDocument6 pagesAssess Patient with Suspected AppendicitisRirin Ajeng Kartiningsih100% (1)
- Case Study: Krizia P. TenerifeDocument8 pagesCase Study: Krizia P. TenerifeKrizia Pandiño TenerifeNo ratings yet
- NCP Acute Pain DiarrheaDocument4 pagesNCP Acute Pain DiarrheaBARRISTERFLOWERSEAURCHIN6No ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationChucky VergaraNo ratings yet
- Assess The Plan To Provide Advice The Advice TheDocument3 pagesAssess The Plan To Provide Advice The Advice TheDarwin QuirimitNo ratings yet
- N220 - Nursing Worksheet: Situation / BackgroundDocument8 pagesN220 - Nursing Worksheet: Situation / BackgroundVivian PhamNo ratings yet
- +care SheetDocument1 page+care SheetVivian PhamNo ratings yet
- Nursing Care Plan: Non-Pharmacological InterventionsDocument4 pagesNursing Care Plan: Non-Pharmacological InterventionsVivian PhamNo ratings yet
- N220 W9 Nursing Care PlanDocument3 pagesN220 W9 Nursing Care PlanVivian PhamNo ratings yet
- N220 W9 Nursing Care PlanDocument3 pagesN220 W9 Nursing Care PlanVivian PhamNo ratings yet
- NRSG Care PlanDocument9 pagesNRSG Care PlanVivian PhamNo ratings yet
- NCP - LeprosyDocument3 pagesNCP - LeprosyKevin DareNo ratings yet
- Urticaria sbd15 PDFDocument16 pagesUrticaria sbd15 PDFBruno Belarmino de QueirozNo ratings yet
- Pediatric NursingDocument187 pagesPediatric NursingNorjetalexis Cabrera100% (1)
- Diabetes Insipidus: Nitha K 2 Year MSC NursingDocument47 pagesDiabetes Insipidus: Nitha K 2 Year MSC NursingNITHA K100% (1)
- E202 Medical Assessment PDFDocument1 pageE202 Medical Assessment PDFSyahidatul Kautsar NajibNo ratings yet
- COVID vaccination certificateDocument2 pagesCOVID vaccination certificateGeorge HonciugNo ratings yet
- Drug StudyDocument12 pagesDrug StudyJessie Cauilan CainNo ratings yet
- Referral Letter for Daniel McCraeDocument3 pagesReferral Letter for Daniel McCraeSi Thi0% (1)
- 365 Daily Health: Natural RemediesDocument16 pages365 Daily Health: Natural RemediesSatish ChandNo ratings yet
- Drug Study AmoxicillinDocument3 pagesDrug Study AmoxicillinJanzelvine Lee MontenegroNo ratings yet
- Platelet Disorders: Autoimmune ThrombocytopeniasDocument6 pagesPlatelet Disorders: Autoimmune ThrombocytopeniasShī Fu KoNo ratings yet
- ENT Educational Objectives U World Step 1Document6 pagesENT Educational Objectives U World Step 1Usama BilalNo ratings yet
- So-So: A Brokerage Will Only Get You FarDocument104 pagesSo-So: A Brokerage Will Only Get You Farenock-readersNo ratings yet
- FMGE March 2008 MCQs Hello Everyone, If The Results AreDocument15 pagesFMGE March 2008 MCQs Hello Everyone, If The Results Arearslansaeed007No ratings yet
- Neuro LogbookDocument16 pagesNeuro Logbookbrunosantiago100% (1)
- Vaginitis in Children (For Parents) - Nemours KidsHealthDocument1 pageVaginitis in Children (For Parents) - Nemours KidsHealthHabtamu tamiruNo ratings yet
- Diagnosis and Treatment of Gestational Trophoblastic Disease PDFDocument11 pagesDiagnosis and Treatment of Gestational Trophoblastic Disease PDFAlexeySAgNo ratings yet
- PEDIATRIC SURGERY - A Comprehensive Textbook For africa.-SPRINGER NATURE (2019) - 631-827Document197 pagesPEDIATRIC SURGERY - A Comprehensive Textbook For africa.-SPRINGER NATURE (2019) - 631-827adhytiyani putriNo ratings yet
- Emergency Department Sepsis PathwayDocument2 pagesEmergency Department Sepsis Pathwaykhoirul anwarNo ratings yet
- Acute Pulmonary EdemaDocument17 pagesAcute Pulmonary EdemaShimmering MoonNo ratings yet
- Subarachnoid Hemorrhage With AneurysymDocument30 pagesSubarachnoid Hemorrhage With AneurysymmunaNo ratings yet
- Clinical Medical Reviews and Case Reports CMRCR 5 227Document8 pagesClinical Medical Reviews and Case Reports CMRCR 5 227Juan BacelarNo ratings yet
- RV Ollero MD's Guide to Advanced Trauma Life SupportDocument18 pagesRV Ollero MD's Guide to Advanced Trauma Life SupportPrincess Cate MercadoNo ratings yet
- Effect of Wound Care Using Robusta Coffee Powders On Diabetic Ulcer Healing in Sekarwangi Hospital SukabumiDocument10 pagesEffect of Wound Care Using Robusta Coffee Powders On Diabetic Ulcer Healing in Sekarwangi Hospital SukabumiBonita SiraitNo ratings yet
- NICU Cheat SheetDocument4 pagesNICU Cheat SheetRichelle FrondaNo ratings yet
- Trombocitopenia Embarazo 2016Document11 pagesTrombocitopenia Embarazo 2016piloricoNo ratings yet
- 8 SquintDocument46 pages8 Squintwanderer_1010No ratings yet
- NCPDocument3 pagesNCPAlexis CoronadoNo ratings yet
- Stroke Society of the Philippines: Guide for Stroke TreatmentDocument22 pagesStroke Society of the Philippines: Guide for Stroke TreatmentSuresh ShresthaNo ratings yet
- Botulinum Toxin InjectionsDocument7 pagesBotulinum Toxin InjectionsWalid YounesNo ratings yet