You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drug StudyDocument13 pagesDrug StudyGi Ey ElNo ratings yet
- CLINICAL Assigmnent 1 PDFDocument12 pagesCLINICAL Assigmnent 1 PDFChelly ClarkeNo ratings yet
- The Aspects of GENE THERAPYDocument12 pagesThe Aspects of GENE THERAPYJasmin Prindiana100% (6)
- Classical Music Therapy As The Intervention To Relieve Headache in ADocument3 pagesClassical Music Therapy As The Intervention To Relieve Headache in AmargaretNo ratings yet
- IP Projects For Class XiiDocument20 pagesIP Projects For Class XiiARATHI THULASINo ratings yet
- Certificate Nowshera Medical Complex Psychiatry Internship CertificateDocument2 pagesCertificate Nowshera Medical Complex Psychiatry Internship CertificateMuhammad Haris Khan KhattakNo ratings yet
- From The SAGE Social Science Collections. All Rights ReservedDocument19 pagesFrom The SAGE Social Science Collections. All Rights ReservedMuhammad Haris Khan KhattakNo ratings yet
- Basic Concepts in Pharmacology1Document24 pagesBasic Concepts in Pharmacology1Muhammad Haris Khan KhattakNo ratings yet
- Interpreting The WAIS-IVDocument45 pagesInterpreting The WAIS-IVMuhammad Haris Khan Khattak100% (1)
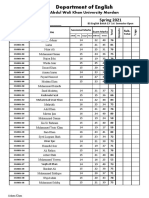
- AWKU English Dept 1st Semester Marks ListDocument8 pagesAWKU English Dept 1st Semester Marks ListMuhammad Haris Khan KhattakNo ratings yet
- Xerox University Microfilms: 300 North Zeeb Road Ann Arbor, Michigan 48106Document427 pagesXerox University Microfilms: 300 North Zeeb Road Ann Arbor, Michigan 48106Muhammad Haris Khan KhattakNo ratings yet
- Psychosis Diagnosis and Antipsychotic Drug TreatmentDocument5 pagesPsychosis Diagnosis and Antipsychotic Drug TreatmentMuhammad Haris Khan KhattakNo ratings yet
- ZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 2Document3 pagesZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 2Muhammad Haris Khan KhattakNo ratings yet
- Hira 40 Lesson PlanDocument122 pagesHira 40 Lesson PlanMuhammad Haris Khan KhattakNo ratings yet
- ZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 4Document7 pagesZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 4Muhammad Haris Khan KhattakNo ratings yet
- ZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 3Document8 pagesZAINAB SHEIKH 01-275192-016 - Assignment-Bahria-Pharmacology 3Muhammad Haris Khan KhattakNo ratings yet
- Hira 40 Lesson PlanDocument122 pagesHira 40 Lesson PlanMuhammad Haris Khan KhattakNo ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentMuhammad Haris Khan KhattakNo ratings yet
- Socratic Dialogue in CBTDocument23 pagesSocratic Dialogue in CBTMuhammad Haris Khan KhattakNo ratings yet
- Psychological First AidDocument75 pagesPsychological First AidMuhammad Haris Khan KhattakNo ratings yet
- IndicatorsDocument2 pagesIndicatorsMuhammad Haris Khan KhattakNo ratings yet
- IndicatorsDocument2 pagesIndicatorsMuhammad Haris Khan KhattakNo ratings yet
- Socratic Dialogue in CBTDocument23 pagesSocratic Dialogue in CBTMuhammad Haris Khan KhattakNo ratings yet
- Socratic Dialogue in CBTDocument23 pagesSocratic Dialogue in CBTMuhammad Haris Khan KhattakNo ratings yet
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentMuhammad Haris Khan KhattakNo ratings yet
- Psychological First AidDocument75 pagesPsychological First AidMuhammad Haris Khan KhattakNo ratings yet
- TestingOnTheInternet PDFDocument72 pagesTestingOnTheInternet PDFMuhammad Haris Khan KhattakNo ratings yet
- Psychological First AidDocument75 pagesPsychological First AidMuhammad Haris Khan KhattakNo ratings yet
- PaperDocument9 pagesPaperMuhammad Haris Khan KhattakNo ratings yet
- TestingOnTheInternet PDFDocument72 pagesTestingOnTheInternet PDFMuhammad Haris Khan KhattakNo ratings yet
- Rumah Sakit Mata ICD X Eng FixDocument11 pagesRumah Sakit Mata ICD X Eng FixPelayanan MedisNo ratings yet
- Wa0013.Document15 pagesWa0013.Simonia CoutinhoNo ratings yet
- Medical Surgical Questions LiverDocument17 pagesMedical Surgical Questions LiverHasan A AsFourNo ratings yet
- Domingo, Precious Mae TDocument56 pagesDomingo, Precious Mae Tbevzie datuNo ratings yet
- New Nursing Diagnoses 2012-2014Document11 pagesNew Nursing Diagnoses 2012-2014CarmenNoemiSantos100% (1)
- Schizophrenia Spectrum and Other Psychotic DisordersDocument8 pagesSchizophrenia Spectrum and Other Psychotic DisordersRain Simonette GuanNo ratings yet
- PEMERINTAH KABUPATN MAMUJU TENGAH DINAS PENDIDIKAN UPTD SMP NEGERI 2 PANGALEDocument4 pagesPEMERINTAH KABUPATN MAMUJU TENGAH DINAS PENDIDIKAN UPTD SMP NEGERI 2 PANGALEFitri ShanumNo ratings yet
- Time TableDocument28 pagesTime TablePetWise Animal ClinicNo ratings yet
- Food Safety: in A State of Transformation: Global Thematic ResearchDocument44 pagesFood Safety: in A State of Transformation: Global Thematic Researchsajid waqasNo ratings yet
- ARTIKEL9 - Jurnal Elective Birth in Twin PregnancyDocument11 pagesARTIKEL9 - Jurnal Elective Birth in Twin PregnancyFarid NurdiansyahNo ratings yet
- Knowledge, Attitude and Practice Towards Malaria Prevention Among School Children Aged 5 - 14 Years in Sub-Saharan Africa - A Review of LiteratureDocument9 pagesKnowledge, Attitude and Practice Towards Malaria Prevention Among School Children Aged 5 - 14 Years in Sub-Saharan Africa - A Review of Literatureemuata ijojo-igboriaNo ratings yet
- Fluid Consumption, Hydration Status and Its Associated Factors - A Cross Sectional Study Among Medical Students in Palembang, IndonesiaDocument36 pagesFluid Consumption, Hydration Status and Its Associated Factors - A Cross Sectional Study Among Medical Students in Palembang, IndonesiaDwi Lisa Nur'ainiNo ratings yet
- Cases in Nephrology by Muhammad Rafiqul AlamDocument9 pagesCases in Nephrology by Muhammad Rafiqul AlamSELLULARNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- LECTURE - 8 Biomaterial PDFDocument34 pagesLECTURE - 8 Biomaterial PDFYoza FendrianiNo ratings yet
- 5 Common Environmental Hazards in The Workplace: Skip To Main ContentDocument48 pages5 Common Environmental Hazards in The Workplace: Skip To Main ContentElvie Rodado GubalaneNo ratings yet
- 665 672Document8 pages665 672Sebastián Ghiso JiménezNo ratings yet
- En VENTIlogic-LS Plus 67781i User ManualDocument125 pagesEn VENTIlogic-LS Plus 67781i User ManualMehmet Ali KaraNo ratings yet
- Urtricaria SDocument8 pagesUrtricaria SpalNo ratings yet
- Analisis Framing Pemberitaan Covid-19 Dimedia Online: KeywordsDocument21 pagesAnalisis Framing Pemberitaan Covid-19 Dimedia Online: Keywordslayla abdullahNo ratings yet
- Occupational Therapy For MNDDocument92 pagesOccupational Therapy For MNDSharifNo ratings yet
- Reduce cholesterol and triglycerides with CRESTORDocument2 pagesReduce cholesterol and triglycerides with CRESTORSunny Mae T. PuigNo ratings yet
- Allied Health ProfessionalsDocument19 pagesAllied Health ProfessionalsReihnard RosariioNo ratings yet
- JC BdiDocument36 pagesJC BdiArisa KudidthalertNo ratings yet
- MEGALOBLASTIC ANAEMIA - pptxsdd.pptx.4Document30 pagesMEGALOBLASTIC ANAEMIA - pptxsdd.pptx.4Hiba MohammedNo ratings yet