You might also like
- Roundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandRoundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Summary of CDC Treatment GuidelinesDocument24 pagesSummary of CDC Treatment GuidelinesJuan MoralesNo ratings yet
- Summary of CDC STI Treatment Guidelines, 2021Document1 pageSummary of CDC STI Treatment Guidelines, 2021Saranya RaviNo ratings yet
- ETS TX OMSDocument24 pagesETS TX OMSAline MirandaNo ratings yet
- 2021 and 2015 CDC STD Treatment Guidelines 9.8.21 FINALDocument3 pages2021 and 2015 CDC STD Treatment Guidelines 9.8.21 FINALVinh ThếNo ratings yet
- Sexually Transmitted Diseases: Summary of CDC Treatment GuidelinesDocument3 pagesSexually Transmitted Diseases: Summary of CDC Treatment GuidelinesbenzveewitNo ratings yet
- Anti-Parasite Drugs: Classification and Treatment OptionsDocument44 pagesAnti-Parasite Drugs: Classification and Treatment OptionsDeanGrestamaNo ratings yet
- Sexually Transmitted Diseases: Summary of CDC Treatment GuidelinesDocument3 pagesSexually Transmitted Diseases: Summary of CDC Treatment GuidelinesSumate KittiNo ratings yet
- PatogenDocument1 pagePatogenMutiara Dita PutriNo ratings yet
- Generic Name Indication Mechanism of Action Classification Side Effects/Adverse Drug Reactions Nursing ResponsibilitiesDocument3 pagesGeneric Name Indication Mechanism of Action Classification Side Effects/Adverse Drug Reactions Nursing ResponsibilitiesNicholas TagleNo ratings yet
- Dr. Anati's Parasitic Diseases and TreatmentsDocument40 pagesDr. Anati's Parasitic Diseases and Treatmentsanes tiraNo ratings yet
- Clinical Practice Guidelines ON Acute Gastro-Enteritis: Santissima Trinidad HospitalDocument3 pagesClinical Practice Guidelines ON Acute Gastro-Enteritis: Santissima Trinidad HospitalEspie FerrerNo ratings yet
- ID SummaryDocument16 pagesID SummarysleeembyNo ratings yet
- MedicinesDocument6 pagesMedicinesMARJINA A. UDDAHNo ratings yet
- Common Opportunistic Infections in HIVDocument3 pagesCommon Opportunistic Infections in HIVjesmitha2740No ratings yet
- Recommended Treatments for Chlamydia and GonorrheaDocument1 pageRecommended Treatments for Chlamydia and GonorrheadoodrillNo ratings yet
- STD ShortDocument1 pageSTD Shortasmatmasoom5566No ratings yet
- Drugs and DosagesDocument40 pagesDrugs and DosagesGeraldine Marie Salvo100% (1)
- Andhika Rezeky Gunawan - Tugas FarmakoDocument4 pagesAndhika Rezeky Gunawan - Tugas FarmakoAndhika gunawanNo ratings yet
- Acyclovir vs. FamvirDocument7 pagesAcyclovir vs. Famvirkobzvnsq814No ratings yet
- Antibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateDocument2 pagesAntibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateKevo VillagranNo ratings yet
- PenyakitDocument2 pagesPenyakitbubigembullNo ratings yet
- Empiric Antibiotic Treatment of Urinary Tract InfectionsDocument3 pagesEmpiric Antibiotic Treatment of Urinary Tract InfectionsVikas KumarNo ratings yet
- Tablet Coamoxiclave (Amoxicillin +clavulanic Acid) Indications and DosDocument2 pagesTablet Coamoxiclave (Amoxicillin +clavulanic Acid) Indications and DosShumaila Iftikhar Iftikhar AhmadNo ratings yet
- AGE (Updated)Document3 pagesAGE (Updated)Sanielle Karla Garcia LorenzoNo ratings yet
- antibiotic policy newDocument2 pagesantibiotic policy newhaliya MakwanaNo ratings yet
- DDS4 PrescriptionsDocument1 pageDDS4 PrescriptionsR MNo ratings yet
- Ciprofloxacin treatment for UTIDocument1 pageCiprofloxacin treatment for UTIWong Lee CheeNo ratings yet
- FloridaSharkman ProtocolsDocument14 pagesFloridaSharkman ProtocolsgurwaziNo ratings yet
- 05 Pharmacology PLE 2019 RatioDocument50 pages05 Pharmacology PLE 2019 RatioPatricia VillegasNo ratings yet
- Antiviral Drugs With Their Route of AdministrationDocument2 pagesAntiviral Drugs With Their Route of AdministrationFerahadin SultanNo ratings yet
- Group 4 LEPTOSPIROSIS DDM 4BDocument43 pagesGroup 4 LEPTOSPIROSIS DDM 4BDaymon, Ma. TeresaNo ratings yet
- Antibiotic dosing guide for adults and childrenDocument2 pagesAntibiotic dosing guide for adults and childrenEduard MilitaruNo ratings yet
- Med MissionDocument3 pagesMed MissionNicole CabahugNo ratings yet
- DosesDocument9 pagesDosesthelordhaniNo ratings yet
- Nama Obat Sediaan Dosis Durasi Pemberian AntibiotikDocument2 pagesNama Obat Sediaan Dosis Durasi Pemberian AntibiotikNurmayra AmrizaNo ratings yet
- Obat UKMPPDDocument54 pagesObat UKMPPDMuh.ikhsan zainalNo ratings yet
- COVID Care Advice Home QuarantineDocument2 pagesCOVID Care Advice Home QuarantineTANMAYA RANJAN BALABANTARAYNo ratings yet
- Prescription Analysis Lab ErrorsDocument16 pagesPrescription Analysis Lab ErrorsReuvenn ObaniNo ratings yet
- COVID home care adviceDocument1 pageCOVID home care adviceSai Krishna Chaitanya AddagallaNo ratings yet
- Giardiasis Causing Both Endemic and Epidemic Intestinal Disease and DiarrheaDocument7 pagesGiardiasis Causing Both Endemic and Epidemic Intestinal Disease and Diarrheanathan asfahaNo ratings yet
- Nepal Essential MedicationsDocument103 pagesNepal Essential MedicationsPriya SahNo ratings yet
- CD ColitisDocument1 pageCD ColitisMohammed IssaNo ratings yet
- Antibiotic ChartsDocument61 pagesAntibiotic Chartspempekplg100% (1)
- Zentel™ Albendazole: Page 1 of 5Document5 pagesZentel™ Albendazole: Page 1 of 5zain qadriNo ratings yet
- ACE Panel Report - Antibiotic Use in Endodontic Infections - FinalDocument1 pageACE Panel Report - Antibiotic Use in Endodontic Infections - FinalMohammed NabeelNo ratings yet
- Drug Brand Name Drug Generic Name Route Dose Dosage Duration SpecificDocument1 pageDrug Brand Name Drug Generic Name Route Dose Dosage Duration SpecificSartaj GillNo ratings yet
- Amoxicillin 125 MG 250 MG 5 ML Oral SuspensionDocument16 pagesAmoxicillin 125 MG 250 MG 5 ML Oral SuspensionAshrafNo ratings yet
- No Golongan Nama Obat Dosis AntibiotikDocument2 pagesNo Golongan Nama Obat Dosis AntibiotikPuspitariniSetyaningsihNo ratings yet
- CellulitisDocument1 pageCellulitisSanielle Karla Garcia LorenzoNo ratings yet
- Antibiotics, steroids, inhalers and moreDocument2 pagesAntibiotics, steroids, inhalers and moreCARES Martin Federic PalcoNo ratings yet
- SDCEP Drug Prescribing Ed 3 Update June 2021Document4 pagesSDCEP Drug Prescribing Ed 3 Update June 2021ABNo ratings yet
- urinary_adultsDocument16 pagesurinary_adultsPaolo MaurelliNo ratings yet
- AB Doses Common DiseasesDocument15 pagesAB Doses Common DiseasesTariqNo ratings yet
- No Nama Indikasi Sediaan Kelas 1 Amoxicillin Tablet: 500mg PenicillinDocument3 pagesNo Nama Indikasi Sediaan Kelas 1 Amoxicillin Tablet: 500mg PenicillinwandawinkyNo ratings yet
- Kumpulan Daftar ObatDocument6 pagesKumpulan Daftar ObatZega AgustianNo ratings yet
- Ciprobay PIDocument26 pagesCiprobay PIfsdfNo ratings yet
- Adult: PO Pain 15-60 MG 4 Hrly. Max: 360 Mg/day. Cough SuppressantDocument13 pagesAdult: PO Pain 15-60 MG 4 Hrly. Max: 360 Mg/day. Cough Suppressantwilliam_SatyanegaraNo ratings yet
- DoxycyclineDocument3 pagesDoxycyclineLynn Marie Igos DelgadoNo ratings yet
- 24 Week Intro Contest CycleDocument1 page24 Week Intro Contest CycleTHIMMAPPANo ratings yet
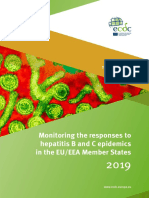
- Hepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019Document87 pagesHepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019neleaNo ratings yet
- Kdigo-Gn-Guideline GN PDFDocument143 pagesKdigo-Gn-Guideline GN PDFFerry JuniansyahNo ratings yet
- Search The Data - Healthy People 2020Document5 pagesSearch The Data - Healthy People 2020neleaNo ratings yet
- Hepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019Document87 pagesHepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019neleaNo ratings yet
- OCDE - Health at A Glance 2019 - 4dd50c09-En PDFDocument243 pagesOCDE - Health at A Glance 2019 - 4dd50c09-En PDFJosé Anselmo de Carvalho JúniorNo ratings yet
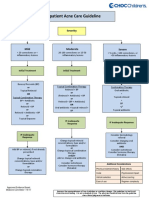
- Outpatient Acne Care Guideline: SeverityDocument5 pagesOutpatient Acne Care Guideline: SeverityMarrauNo ratings yet
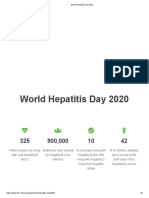
- World Hepatitis Day 2020Document2 pagesWorld Hepatitis Day 2020neleaNo ratings yet
- Hepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019Document87 pagesHepatitis B C Monitoring Responses Hepatitis B C Epidemics EU EEA Member States 2019neleaNo ratings yet
- OCDE - Health at A Glance 2019 - 4dd50c09-En PDFDocument243 pagesOCDE - Health at A Glance 2019 - 4dd50c09-En PDFJosé Anselmo de Carvalho JúniorNo ratings yet
- Manual de Utilizare ClasaB 2010Document296 pagesManual de Utilizare ClasaB 2010neleaNo ratings yet
- OCDE - Health at A Glance 2019 - 4dd50c09-En PDFDocument243 pagesOCDE - Health at A Glance 2019 - 4dd50c09-En PDFJosé Anselmo de Carvalho JúniorNo ratings yet
- Personal Hygiene: How To Keep Your Body CleanDocument13 pagesPersonal Hygiene: How To Keep Your Body CleanneleaNo ratings yet
- Get PDF - Calcipotriol Ointment in Nail Psoriasis - A Controlled Double-Blind Comparison With Betamethasone Dipropionate and Salicylic AcidDocument1 pageGet PDF - Calcipotriol Ointment in Nail Psoriasis - A Controlled Double-Blind Comparison With Betamethasone Dipropionate and Salicylic AcidneleaNo ratings yet
- Systematic Review Hepatitis B C PrevalenceDocument133 pagesSystematic Review Hepatitis B C PrevalenceneleaNo ratings yet
- Table 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)Document2 pagesTable 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)neleaNo ratings yet
- JDV 13776Document8 pagesJDV 13776Cristian MaresNo ratings yet
- vvc-2019 UkDocument46 pagesvvc-2019 UkneleaNo ratings yet
- Titlu Ghid AcneDocument1 pageTitlu Ghid AcneneleaNo ratings yet
- Loss-Of-Function Mutations in CARD14 Are Associated With A Severe Variant of Atopic DermatitisDocument20 pagesLoss-Of-Function Mutations in CARD14 Are Associated With A Severe Variant of Atopic DermatitisneleaNo ratings yet
- A Controlled Study of Comparative e Cacy of Oral Retinoid and Topical Betamethasone/salicylic Acid For Chronic Hyperkeratotic Palmoplantar DermatitisDocument2 pagesA Controlled Study of Comparative e Cacy of Oral Retinoid and Topical Betamethasone/salicylic Acid For Chronic Hyperkeratotic Palmoplantar DermatitisneleaNo ratings yet
- Safety and Efficacy of Quadriderme® in The Treatment of Impetiginous Eczema (Study P05134AM4)Document11 pagesSafety and Efficacy of Quadriderme® in The Treatment of Impetiginous Eczema (Study P05134AM4)neleaNo ratings yet
- Triderm - DRRCP 2010 BelgiumDocument6 pagesTriderm - DRRCP 2010 BelgiumneleaNo ratings yet
- "Outside-to-Inside" (And Now Back To "Outside") Pathogenic Mechanisms in Atopic DermatitisDocument8 pages"Outside-to-Inside" (And Now Back To "Outside") Pathogenic Mechanisms in Atopic DermatitisneleaNo ratings yet
- Derm 2016 Bun PrepDocument596 pagesDerm 2016 Bun PrepneleaNo ratings yet
- DiDomenico 2018-ADDocument14 pagesDiDomenico 2018-ADneleaNo ratings yet
- DiDomenico 2018-ADDocument14 pagesDiDomenico 2018-ADneleaNo ratings yet
- Derm 2016 Bun PrepDocument596 pagesDerm 2016 Bun PrepneleaNo ratings yet
- Mrsa MssaDocument6 pagesMrsa MssaneleaNo ratings yet
- Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and ComplicationsDocument35 pagesDiagnosis of Atopic Dermatitis: Mimics, Overlaps, and ComplicationsneleaNo ratings yet
- Huikahi Restorative CirclesDocument6 pagesHuikahi Restorative CirclesCarl Vincent QuitorianoNo ratings yet
- Perception of Covid-19 and Acceptance of Vaccination in Delta State NigeriaDocument27 pagesPerception of Covid-19 and Acceptance of Vaccination in Delta State NigeriaBlessing O. JosiahNo ratings yet
- The Last Sheet.: Ronnie D. Caringal Canubing National High SchoolDocument57 pagesThe Last Sheet.: Ronnie D. Caringal Canubing National High SchoolVICKY HERMOSURANo ratings yet
- CBT Exam To PrintDocument55 pagesCBT Exam To Printdoreen pestanoNo ratings yet
- Community Medicine: Cross-Sectional Studies (Prevalence Studies/ Surveys)Document5 pagesCommunity Medicine: Cross-Sectional Studies (Prevalence Studies/ Surveys)api-3829364No ratings yet
- 147-Article Text-580-1-10-20211119Document12 pages147-Article Text-580-1-10-20211119PreaNo ratings yet
- Sripal Vaccine CertificateDocument2 pagesSripal Vaccine CertificateGyan Pratap SinghNo ratings yet
- Dengue Infection AdvancesDocument2 pagesDengue Infection AdvancesMAY JOY MARQUEZNo ratings yet
- Discharge TB Summary CensusDocument5 pagesDischarge TB Summary CensusEdryl Piamonte UgpoNo ratings yet
- 2019 Clinical Guidelines SummaryDocument2 pages2019 Clinical Guidelines SummaryEddie WyattNo ratings yet
- Cardiologist Prof Rishi Sethi' Presentation On World Heart DayDocument36 pagesCardiologist Prof Rishi Sethi' Presentation On World Heart DaybobbyramakantNo ratings yet
- Health Safety in Oil Gas SectorDocument50 pagesHealth Safety in Oil Gas SectorSaid Amayyas AmazighNo ratings yet
- International Health OverviewDocument46 pagesInternational Health Overviewmatt medmedmedic100% (1)
- Background of The StudyDocument5 pagesBackground of The StudyDave PeriaNo ratings yet
- MultipLa - A Tool For The Combined Overall Estimation of Various Types of MMHDocument3 pagesMultipLa - A Tool For The Combined Overall Estimation of Various Types of MMHAfirdie FirdausNo ratings yet
- Wound DressingDocument1 pageWound DressingApurba Dey100% (2)
- Anganwadi Sanitation: UnicefDocument25 pagesAnganwadi Sanitation: UnicefRachit AgarwalNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanMeryl MarcosNo ratings yet
- NCM 109 LEC Alterations With Infectious Inflammatory and Immunologic Responses PDFDocument18 pagesNCM 109 LEC Alterations With Infectious Inflammatory and Immunologic Responses PDFcalliemozartNo ratings yet
- Relationship between patient characteristics, risky behavior, STIs and HIV/AIDS incidentsDocument22 pagesRelationship between patient characteristics, risky behavior, STIs and HIV/AIDS incidentsQorryNo ratings yet
- BrochureDocument2 pagesBrochureapi-238213388No ratings yet
- COVID-19: Impacts and OpportunitiesDocument21 pagesCOVID-19: Impacts and OpportunitiesCityNewsTorontoNo ratings yet
- Menstruation 101: A Guide to Your First Period and Period CareDocument8 pagesMenstruation 101: A Guide to Your First Period and Period CareSheeba StalinNo ratings yet
- Presentation Progress and Status of Consulting Services ContractDocument26 pagesPresentation Progress and Status of Consulting Services ContractDjoko SubektiNo ratings yet
- CholeraDocument4 pagesCholeraJoanne Kaye TaylorNo ratings yet
- Comprehensive Abortion Care GuideDocument42 pagesComprehensive Abortion Care GuideKate SantosNo ratings yet
- Sanitation Standard Operating ProcedureDocument6 pagesSanitation Standard Operating ProcedureCatherine Jane CallangaNo ratings yet
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving PassengersKoteswar MandavaNo ratings yet
- Haccp Rumah Sakit Jurnal KesehatanDocument8 pagesHaccp Rumah Sakit Jurnal KesehatanYohanes KristiantoNo ratings yet
- India's Health Committees Guide National PlanningDocument94 pagesIndia's Health Committees Guide National Planningmidhum mNo ratings yet