You might also like
- NCP Violence - OtherDocument2 pagesNCP Violence - OtherRosean Venus SilangNo ratings yet
- Mrs. Ma. Lourdes B. Domingo, RNDocument3 pagesMrs. Ma. Lourdes B. Domingo, RNRomzy BasañesNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNeza AgdalesNo ratings yet
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline ChaNo ratings yet
- Severe Anxiety As Evidenced by Repetitive ActionDocument1 pageSevere Anxiety As Evidenced by Repetitive ActionRomzy Basañes100% (3)
- Nursing CARE PLAN PsychDocument7 pagesNursing CARE PLAN Psychtiptopyo100% (1)
- NCP For ConcussionDocument3 pagesNCP For Concussiontamtam_antonio100% (1)
- Disturbed Visual Sensory Perception Related: Nursing Care PlanDocument3 pagesDisturbed Visual Sensory Perception Related: Nursing Care PlanMae Therese B. MAGNONo ratings yet
- NCP Cataract SurgeryDocument5 pagesNCP Cataract SurgeryKristaJaneCelmarBagcatNo ratings yet
- Hypothyroidism Nursing Care PlanDocument3 pagesHypothyroidism Nursing Care PlanRizza Mae MaglacionNo ratings yet
- Cva NCP AnxietyDocument1 pageCva NCP AnxietyQueenElsaDeVeraNo ratings yet
- OCD NCPDocument2 pagesOCD NCPkharla suriaga100% (1)
- Homework - Anxiety Nursing Care PlanDocument2 pagesHomework - Anxiety Nursing Care PlanmonaNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- Nursing Care Plan Impaired AdjustmentDocument1 pageNursing Care Plan Impaired Adjustmentderic100% (2)
- Cystic Fibrosis Nursing Care PlanDocument15 pagesCystic Fibrosis Nursing Care PlanAira Anne Tonee VillaminNo ratings yet
- System Normal Abnormal Remarks Vital SignsDocument3 pagesSystem Normal Abnormal Remarks Vital SignsJM RomiasNo ratings yet
- Delayed Growth NCPDocument3 pagesDelayed Growth NCPPau-pau BasiNo ratings yet
- NCP LocDocument2 pagesNCP LocMel RodolfoNo ratings yet
- Hearing Loss in Older AdultsDocument2 pagesHearing Loss in Older AdultsFran Lan100% (1)
- Nursing Assessment Objectives and Intervention for ConjunctivitisDocument2 pagesNursing Assessment Objectives and Intervention for ConjunctivitisIna Marie Calungcaguin Castro100% (1)
- AcetazolamideDocument3 pagesAcetazolamideGwyn RosalesNo ratings yet
- Alzheimers Nursing Care PlanDocument6 pagesAlzheimers Nursing Care Planmp1757100% (1)
- Drug Tabulation orDocument23 pagesDrug Tabulation orChin Villanueva UlamNo ratings yet
- NCP ChoreaDocument4 pagesNCP Choreanj_pink081794100% (2)
- Nursing Care Plan: Phinma University of IloiloDocument4 pagesNursing Care Plan: Phinma University of IloiloLestly Mae Tedios MongayaNo ratings yet
- NCP For CHDDocument2 pagesNCP For CHDMonica Rivera100% (1)
- NCP SviDocument4 pagesNCP SviEjie Boy IsagaNo ratings yet
- Self Care DeficitDocument4 pagesSelf Care DeficitEllaine RamirezNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care Plankreny1050% (2)
- 05 NCP - Drug StudyDocument23 pages05 NCP - Drug StudyRene John FranciscoNo ratings yet
- Nursing Care Plan For DepressionDocument7 pagesNursing Care Plan For DepressionCatherineNo ratings yet
- NCP - Major Depressive DisorderDocument7 pagesNCP - Major Depressive DisorderJaylord Verazon100% (1)
- NCP Otitis MediaDocument2 pagesNCP Otitis MediaHanz Alec100% (2)
- Gender Dysphoria NCPDocument1 pageGender Dysphoria NCPSeann LorescoNo ratings yet
- Nursing Management of Patients With DementiaDocument9 pagesNursing Management of Patients With DementiaSabita Paudel60% (5)
- Hizon 2 NCP 1 Npi I Am SamDocument5 pagesHizon 2 NCP 1 Npi I Am SamDan HizonNo ratings yet
- Nursing Care Plan: Short Term: Independent: Independent: Short TermDocument6 pagesNursing Care Plan: Short Term: Independent: Independent: Short TermSittie Sobaidah D. DimakutaNo ratings yet
- Teaching P UlcersDocument2 pagesTeaching P UlcersFiona Cheryl Amsterdam100% (1)
- Improving Comfort with Endotracheal TubeDocument1 pageImproving Comfort with Endotracheal TubeSelwynVillamorPatenteNo ratings yet
- Nursing Diagnosis and InterventionsDocument4 pagesNursing Diagnosis and InterventionsCharley DegamoNo ratings yet
- Rationale: This Will Assess Pain LevelDocument7 pagesRationale: This Will Assess Pain LevelCoreyNo ratings yet
- Assessment Diagnosis Planning Implimentation Rationale ResponseDocument4 pagesAssessment Diagnosis Planning Implimentation Rationale Responsekhate fonteNo ratings yet
- Acetylcysteine NACDocument2 pagesAcetylcysteine NACKristine YoungNo ratings yet
- Cleft Lip Palate NCPDocument2 pagesCleft Lip Palate NCPLerma PagcaliwanganNo ratings yet
- Nursing Care Plan For Pneumonia NCP PDFDocument3 pagesNursing Care Plan For Pneumonia NCP PDFFARAH MAE MEDINA100% (2)
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- Intussusception Nursing Care PlanDocument7 pagesIntussusception Nursing Care PlanElli SuñgaNo ratings yet
- Drug StudyDocument4 pagesDrug Studyreanne_davidNo ratings yet
- Crisis Intervention: Psychiatric Nursing Nursing Care PlanDocument13 pagesCrisis Intervention: Psychiatric Nursing Nursing Care PlanKatherine 'Chingboo' Leonico Laud100% (4)
- Nursing Care Plan GlaucomaDocument3 pagesNursing Care Plan Glaucomasephirus77750% (4)
- Caring for an Elderly Patient with DepressionDocument2 pagesCaring for an Elderly Patient with DepressionSheryl Ann Barit PedinesNo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Anxiety Related To Stress HspitaiztionDocument1 pageAnxiety Related To Stress HspitaiztionEunice Lan Sandoval Ardiente100% (3)
- Nursing Care Plan - HyperDocument4 pagesNursing Care Plan - HyperJennalyn Casapao100% (1)
- Orbital Trauma NCP and Drug StudyDocument5 pagesOrbital Trauma NCP and Drug StudyDersly LaneNo ratings yet
- NURSING CARE PLAN For Myocardial InfarctionDocument16 pagesNURSING CARE PLAN For Myocardial InfarctionFreisanChenMandumotan100% (1)
- Principles of Pathophysiology - Bullock, ShaneDocument2 pagesPrinciples of Pathophysiology - Bullock, ShaneMel Izhra N. MargateNo ratings yet
- Nursing Assessment and Interventions for Acute Chest PainDocument3 pagesNursing Assessment and Interventions for Acute Chest PainAjay SupanNo ratings yet
- NCPsDocument13 pagesNCPsdarwinNo ratings yet
- Placenta Accreta (Or Worse!) : Deward Voss, MD James Pavelka, MDDocument75 pagesPlacenta Accreta (Or Worse!) : Deward Voss, MD James Pavelka, MDYessamin Paith RoderosNo ratings yet
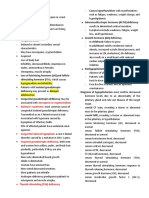
- Micropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyDocument4 pagesMicropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyYessamin Paith RoderosNo ratings yet
- April 12Document1 pageApril 12Yessamin Paith RoderosNo ratings yet
- Language, Orientation, Memory, Attention Span and Calculation, LOCDocument7 pagesLanguage, Orientation, Memory, Attention Span and Calculation, LOCYessamin Paith RoderosNo ratings yet
- Physical Injuries (WHEN TO SUSPECT ABUSE) Role Recognizing Recording Referring Reporting PreventingDocument31 pagesPhysical Injuries (WHEN TO SUSPECT ABUSE) Role Recognizing Recording Referring Reporting PreventingYessamin Paith RoderosNo ratings yet
- Case Study Number FourDocument5 pagesCase Study Number FourYessamin Paith RoderosNo ratings yet
- How To Start A Youth Pastoral PlanningDocument3 pagesHow To Start A Youth Pastoral PlanningYessamin Paith RoderosNo ratings yet
- Problem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemDocument2 pagesProblem: Diabetes Mellitus: Criteria Computation Actual Score Justification I. Nature of The ProblemYessamin Paith RoderosNo ratings yet
- Corona Virus - 19: A Case PresentationDocument25 pagesCorona Virus - 19: A Case PresentationYessamin Paith RoderosNo ratings yet
- College of Nursing: City of Malolos, BulacanDocument255 pagesCollege of Nursing: City of Malolos, BulacanYessamin Paith RoderosNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument8 pagesChronic Obstructive Pulmonary DiseaseYessamin Paith RoderosNo ratings yet
- No Proper DrainageDocument7 pagesNo Proper DrainageYessamin Paith RoderosNo ratings yet
- Risk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Document2 pagesRisk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Yessamin Paith Roderos100% (1)
- Case Study Number FourDocument5 pagesCase Study Number FourYessamin Paith RoderosNo ratings yet
- C. Home and Environment: 1 Year 13%Document8 pagesC. Home and Environment: 1 Year 13%Yessamin Paith RoderosNo ratings yet
- A. Community Health Assessment Tools: Nursing Process in The Care of Population Groups and CommunityDocument4 pagesA. Community Health Assessment Tools: Nursing Process in The Care of Population Groups and CommunityYessamin Paith RoderosNo ratings yet
- CHN ExamDocument35 pagesCHN ExamYessamin Paith RoderosNo ratings yet
- C. Home and Environment: 1 Year 13%Document8 pagesC. Home and Environment: 1 Year 13%Yessamin Paith RoderosNo ratings yet
- Brain Abscess (MEDSURG)Document3 pagesBrain Abscess (MEDSURG)Yessamin Paith RoderosNo ratings yet
- Activity 1: Full Name: Subject: Evidence Based Nursing General QuestionDocument1 pageActivity 1: Full Name: Subject: Evidence Based Nursing General QuestionYessamin Paith RoderosNo ratings yet
- IOTA - International - 2019 - Observership - Program 3 PDFDocument3 pagesIOTA - International - 2019 - Observership - Program 3 PDFJose Eduardo QuinteroNo ratings yet
- نصايحHistopathology FRCPath part 2 exam prepation advice (Ranya) (1) Document3 pagesنصايحHistopathology FRCPath part 2 exam prepation advice (Ranya) (1) Marvi UmairNo ratings yet
- State of The County Address.Document28 pagesState of The County Address.Kiambu County Government -Kenya.No ratings yet
- BIOETHICSDocument2 pagesBIOETHICSYLA KATRINA BONILLANo ratings yet
- OTC Drug Survey Final ProjectDocument37 pagesOTC Drug Survey Final ProjectAishwaryaNo ratings yet
- Drug Induced Intracranial Hypertension: A Systematic Review and Critical Assessment of Drug Induced CausesDocument10 pagesDrug Induced Intracranial Hypertension: A Systematic Review and Critical Assessment of Drug Induced CausesSerque777No ratings yet
- Latest Pharmacy & Medical BooksDocument7 pagesLatest Pharmacy & Medical BooksKlutz4LifeNo ratings yet
- Medical Rep QuestionsDocument14 pagesMedical Rep Questionshina100% (1)
- Ob NCP 2Document2 pagesOb NCP 2Kimberly Mondala (SHS)No ratings yet
- BNF 65 Information Sheet PDFDocument2 pagesBNF 65 Information Sheet PDFobaidaaljobory100% (1)
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- Test Bank For Fundamentals of Case Management Practice Skills For The Human Services 5th EditionDocument5 pagesTest Bank For Fundamentals of Case Management Practice Skills For The Human Services 5th EditionMonica Degan100% (30)
- KTHDocument12 pagesKTHAli FrhdNo ratings yet
- Maltreatment of Children With DisabilitiesDocument13 pagesMaltreatment of Children With DisabilitiesCatarina GrandeNo ratings yet
- Missed questions on drugs and alcoholDocument4 pagesMissed questions on drugs and alcoholmelodyfathiNo ratings yet
- Code of Ethics for Midwives (CEMDocument15 pagesCode of Ethics for Midwives (CEMMariaCon FloresColumbresNo ratings yet
- Poster ProjectDocument1 pagePoster Projectapi-291204444No ratings yet
- Overcoming barriers to universal healthcare in IndiaDocument2 pagesOvercoming barriers to universal healthcare in India@nshu_theachieverNo ratings yet
- RCA October 2021MRCGP Casebook 3Document1 pageRCA October 2021MRCGP Casebook 3Usm LeeNo ratings yet
- Nejmoa1506110 AppendixDocument77 pagesNejmoa1506110 Appendixdwi purwantiNo ratings yet
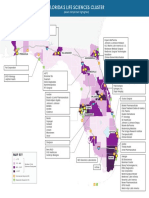
- Florida's Life Sciences Cluster MapDocument1 pageFlorida's Life Sciences Cluster MapCocoNo ratings yet
- IV Therapy Article For ExamDocument10 pagesIV Therapy Article For ExamHui HuangNo ratings yet
- Hospital DelhiDocument18 pagesHospital DelhiKundan KumarNo ratings yet
- nuRSING rEVIEWER PART 2Document9 pagesnuRSING rEVIEWER PART 2Johny VillanuevaNo ratings yet
- MBBS Curriculum 1st Revision 2014 15122014Document478 pagesMBBS Curriculum 1st Revision 2014 15122014gangadharpath123100% (1)
- Stability Considerations For Generic Drugs (PDF - 440KB)Document22 pagesStability Considerations For Generic Drugs (PDF - 440KB)Drx Suraj SinghNo ratings yet
- Namibia Tuberculosis Disease Prevalence Survey Report 2019Document113 pagesNamibia Tuberculosis Disease Prevalence Survey Report 2019Jikan Wa IyasuNo ratings yet
- Suggestions To Improve The Health SectorDocument5 pagesSuggestions To Improve The Health SectorRana Sami100% (1)
- Hazard Ratio.Document13 pagesHazard Ratio.Ali GhanemNo ratings yet
- Practice Bulletins No. 139 - Premature Rupture of Membranes.Document13 pagesPractice Bulletins No. 139 - Premature Rupture of Membranes.Maverick 18100% (1)