You might also like
- pp2 Submission FormatDocument4 pagespp2 Submission Formatapi-314413672No ratings yet
- Traumatic Brain Injury - TBI Medication ChartDocument5 pagesTraumatic Brain Injury - TBI Medication ChartPNo ratings yet
- Aphasia: Hana Nabila Ulfia 1102014118Document14 pagesAphasia: Hana Nabila Ulfia 1102014118hana nabilaNo ratings yet
- CS Lecture1 TBI Introduction 202122 1Document68 pagesCS Lecture1 TBI Introduction 202122 1Vicky TangNo ratings yet
- Jim DX Report RedactedDocument3 pagesJim DX Report Redactedapi-543869960No ratings yet
- Approach To The Patient With AphasiaDocument78 pagesApproach To The Patient With Aphasiasurafel0% (1)
- Differential Diagnosis DysarthriaDocument1 pageDifferential Diagnosis DysarthriaShruti KumarNo ratings yet
- Quick Aphasia Battery (QAB) : 1. Level of ConsciousnessDocument39 pagesQuick Aphasia Battery (QAB) : 1. Level of ConsciousnessomeraNo ratings yet
- Flaccid DysarthriaDocument40 pagesFlaccid Dysarthriaaleeza nomanNo ratings yet
- Aphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpDocument4 pagesAphasia Short Term Goals Long Term Goals Evaluation Assessment WriteUpTarienNo ratings yet
- AphasiaDocument14 pagesAphasiahafida rayni100% (1)
- AphasiaDocument8 pagesAphasiaapi-308647214No ratings yet
- Objetivos ICF-Speech-Sound-Disorder (ASHA)Document2 pagesObjetivos ICF-Speech-Sound-Disorder (ASHA)labavillaNo ratings yet
- Language - NeuroDocument15 pagesLanguage - NeuroAifa Afeeqa Jamilan100% (1)
- Habla ClaraDocument14 pagesHabla ClaraCristóbal Landeros TorresNo ratings yet
- Aphasia, Apraxia, and Agnosia AphasiaDocument7 pagesAphasia, Apraxia, and Agnosia Aphasiasomebody_maNo ratings yet
- AphasiaDocument67 pagesAphasiaIrahmal IrahmalNo ratings yet
- Parkinson's Disease: A Review: Neurology India March 2018Document11 pagesParkinson's Disease: A Review: Neurology India March 2018Alina Vitali TabarceaNo ratings yet
- Post Stroke WritingDocument9 pagesPost Stroke WritingAdi ParamarthaNo ratings yet
- Cerebral Palsy - Critical Elements of Care 6 - 2011Document25 pagesCerebral Palsy - Critical Elements of Care 6 - 2011abdalsucsNo ratings yet
- 2014mshahandouts StoeckelDocument37 pages2014mshahandouts StoeckelAna Vogeley100% (1)
- DysarthriaDocument2 pagesDysarthriaBanjo VergaraNo ratings yet
- 2016 Duffy JR - Motor Speech Disorders Where Will We BeDocument6 pages2016 Duffy JR - Motor Speech Disorders Where Will We BeCarol TibaduizaNo ratings yet
- Cerebral Palsy Brain ParalysisDocument14 pagesCerebral Palsy Brain ParalysisPutri Nindi SNo ratings yet
- Dysarthria AssessmentDocument11 pagesDysarthria AssessmentvviraaNo ratings yet
- Management For Multiple HandicapDocument57 pagesManagement For Multiple HandicapMSc Audio BNo ratings yet
- Cilt HandoutDocument4 pagesCilt Handoutapi-454269640No ratings yet
- Crossed AphasiaDocument5 pagesCrossed AphasiaBeny RiliantoNo ratings yet
- Acute Ischemic Stroke PDFDocument2 pagesAcute Ischemic Stroke PDFXentur XenNo ratings yet
- Classification of Velopharyngeal DysfunctionDocument1 pageClassification of Velopharyngeal DysfunctionVictoria Rojas AlvearNo ratings yet
- Physical Therapy and Occupational Therapy in Parkinson S DiseaseDocument15 pagesPhysical Therapy and Occupational Therapy in Parkinson S DiseaseGerman BuyattiNo ratings yet
- Swallow Screening ToolDocument1 pageSwallow Screening Toolidris LajideNo ratings yet
- HBSE 3303 Dysarthria & ApraxiaDocument4 pagesHBSE 3303 Dysarthria & ApraxiasohaimimohdyusoffNo ratings yet
- Aphasia 07Document34 pagesAphasia 07razik89No ratings yet
- Behavioural Observation AudiometryDocument4 pagesBehavioural Observation AudiometrydarsunaddictedNo ratings yet
- Voice 12345Document36 pagesVoice 12345Vedashri1411No ratings yet
- Chapter-2: Mechanism of Speech Production and Literature ReviewDocument13 pagesChapter-2: Mechanism of Speech Production and Literature ReviewMarixanne Niña Roldan ManzanoNo ratings yet
- Cognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KDocument47 pagesCognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KSureaka PonnusamyNo ratings yet
- Dysarthria ChartDocument12 pagesDysarthria ChartTalia Garcia100% (1)
- AphasiaDocument18 pagesAphasiaVenkatesan VidhyaNo ratings yet
- SB - Pediatrict Vocal NoduleDocument7 pagesSB - Pediatrict Vocal NodulemediNo ratings yet
- Diseases of Esophagus.Document3 pagesDiseases of Esophagus.Isabel Castillo100% (2)
- Hoarseness of VoiceDocument6 pagesHoarseness of VoiceJayantiNo ratings yet
- Aca - 1Document28 pagesAca - 1Aparna LVNo ratings yet
- TxreportmulticulturalDocument4 pagesTxreportmulticulturalapi-294798019No ratings yet
- Western Aphasia Battery Revised Pearson Clinical NaDocument4 pagesWestern Aphasia Battery Revised Pearson Clinical NaBryan Kagz0% (1)
- ORLADocument10 pagesORLACarol CoelhoNo ratings yet
- CfyresumeDocument2 pagesCfyresumeapi-401014427No ratings yet
- Joseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)Document531 pagesJoseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)szeho chanNo ratings yet
- 10 Evoked+potentialDocument6 pages10 Evoked+potentialMahesh RatheeshNo ratings yet
- Non-Speech Oro-Motor Exercises in Post-Stroke Dysarthria Intervention PDFDocument16 pagesNon-Speech Oro-Motor Exercises in Post-Stroke Dysarthria Intervention PDFhgood1001No ratings yet
- AphasiaDocument29 pagesAphasiaHannan FarooqNo ratings yet
- Proforma For Fluency Disorders / KUNNAMPALLIL GEJODocument2 pagesProforma For Fluency Disorders / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- NursingBedsideSwallowingScreen PDFDocument1 pageNursingBedsideSwallowingScreen PDFLUCASNo ratings yet
- Apraxia TestDocument6 pagesApraxia TestRaluca LupuNo ratings yet
- Neuro Behavior DisordersDocument80 pagesNeuro Behavior Disordersmohamadafif_drNo ratings yet
- An Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisDocument6 pagesAn Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisSaranya N MuthuNo ratings yet
- Aphasia: Dr. Ika Marlia, M.SC, Sps Bagian/Smf Neurologi FK Unsyiah/Rsud DR Zainoel Abidin Banda AcehDocument14 pagesAphasia: Dr. Ika Marlia, M.SC, Sps Bagian/Smf Neurologi FK Unsyiah/Rsud DR Zainoel Abidin Banda AcehRudy LusmiandaNo ratings yet
- Hyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Speak Out and Loud Crowd Training CertificateDocument1 pageSpeak Out and Loud Crowd Training Certificateapi-557136848No ratings yet
- Olivia Withrow: The Mbsimp Reliability Zone Has Been Completed byDocument1 pageOlivia Withrow: The Mbsimp Reliability Zone Has Been Completed byapi-557136848No ratings yet
- Multimodal Aphasia TherapiesDocument27 pagesMultimodal Aphasia Therapiesapi-557136848No ratings yet
- Rip ProjectDocument7 pagesRip Projectapi-557136848No ratings yet
- Special Populations HandoutDocument1 pageSpecial Populations Handoutapi-557136848No ratings yet
- Integrated Phonological Awareness ApproachDocument11 pagesIntegrated Phonological Awareness Approachapi-557136848No ratings yet
- Unofficial Academic Transcipt Undergraduate and GraduateDocument7 pagesUnofficial Academic Transcipt Undergraduate and Graduateapi-557136848No ratings yet
- HEALTH DECLARATION of GRADE 5 JASMINDocument3 pagesHEALTH DECLARATION of GRADE 5 JASMINPRINCESS BALISINo ratings yet
- Palate.: Dental Velar Labiodenta LDocument9 pagesPalate.: Dental Velar Labiodenta LHong Ho50% (2)
- Icd 9 10 THTDocument33 pagesIcd 9 10 THTAJENG DWINo ratings yet
- Voice ArticulationDocument4 pagesVoice Articulationsharmaine barjaNo ratings yet
- Acoustic Passaggio Pedagogy For The Male PDFDocument6 pagesAcoustic Passaggio Pedagogy For The Male PDFFernando Vidal Flores SarmientoNo ratings yet
- Vocal ResonanceDocument2 pagesVocal ResonanceDr Daniel K. RobinsonNo ratings yet
- qb19 - Media Notes - Am A-L PDFDocument171 pagesqb19 - Media Notes - Am A-L PDFHarry CramerNo ratings yet
- Skripsi Fitri Sakinah - UNAND 2017Document92 pagesSkripsi Fitri Sakinah - UNAND 2017ririen refrina sariNo ratings yet
- Logbook: Amcmet Medical College AHMEDABAD-380008 Gujarat, IndiaDocument43 pagesLogbook: Amcmet Medical College AHMEDABAD-380008 Gujarat, IndiaShonaNo ratings yet
- Choral Pedagogy and Vocal HealthDocument7 pagesChoral Pedagogy and Vocal Healthradamir100% (1)
- ASHA Required Skills in ARDocument22 pagesASHA Required Skills in AROmar NaimatNo ratings yet
- Makalah Phonology Kelompok 2Document11 pagesMakalah Phonology Kelompok 2meldianto manugalaNo ratings yet
- Careers in Surgery 2014Document27 pagesCareers in Surgery 2014Josue Gabriel da CostaNo ratings yet
- 1 Ugc-Hrd Hearing & SpeechDocument72 pages1 Ugc-Hrd Hearing & SpeechKamal SinghNo ratings yet
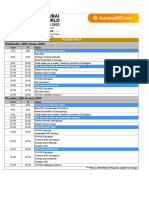
- Ifos 2023 Yo Ifos TrackDocument3 pagesIfos 2023 Yo Ifos TrackAhmad NawazNo ratings yet
- Comprehensive Specialities With The Finest Consultants: MBBS, MD (O&G), MrcogDocument2 pagesComprehensive Specialities With The Finest Consultants: MBBS, MD (O&G), MrcogAshique AkbarNo ratings yet
- Meniere DiseaseDocument6 pagesMeniere Diseasefirza yoga baskoroNo ratings yet
- SPHY303 Week 1 Clinical Classification of Voice Disorders (3 Slides)Document7 pagesSPHY303 Week 1 Clinical Classification of Voice Disorders (3 Slides)TimNo ratings yet
- Otorrino P2Document93 pagesOtorrino P2karlavalenciaalayolaNo ratings yet
- ENT MneumonicDocument4 pagesENT MneumonicVolksWongsathornNo ratings yet
- AAOHNS MembershipApplicationDocument4 pagesAAOHNS MembershipApplicationAnonymous AuJncFVWvNo ratings yet
- Comprehensive Board Exam ENT PDFDocument644 pagesComprehensive Board Exam ENT PDFdrskbarla50% (2)
- A Rare Case Report: Ayurvedic Management of Vocal Cord NodulesDocument4 pagesA Rare Case Report: Ayurvedic Management of Vocal Cord NodulesCindy AmaliaNo ratings yet
- SVC Referring Doctors Booklet 2018 2019Document84 pagesSVC Referring Doctors Booklet 2018 2019keerthi.sakthi0794No ratings yet
- Nasal Angiofibroma in A Female: A Rare Case Report: OtolaryngologyDocument2 pagesNasal Angiofibroma in A Female: A Rare Case Report: OtolaryngologyKhumaira SantaNo ratings yet
- Non Organic Hearing LossDocument59 pagesNon Organic Hearing LossAakritiNo ratings yet
- Hearing Thresholds With Outer and Inner Hair Cell LossDocument13 pagesHearing Thresholds With Outer and Inner Hair Cell LossMarco FioriniNo ratings yet
- Reflux Symptom IndexDocument3 pagesReflux Symptom IndexyenyenNo ratings yet
- Woc ArdsDocument2 pagesWoc Ardssyarifah salmaNo ratings yet
- LPR Its Not GerdDocument3 pagesLPR Its Not GerdWilhelm HeinleinNo ratings yet