You might also like
- NRPH AlgoDocument13 pagesNRPH AlgoJm Jm100% (1)
- Exploring Science Active Book 8Document58 pagesExploring Science Active Book 8Raistlin Chan Ching Kit50% (2)
- Airway Obstruction and VentilationDocument8 pagesAirway Obstruction and VentilationJeremias KwapiszNo ratings yet
- Optiflow Presentation-Carly TorgersenDocument12 pagesOptiflow Presentation-Carly Torgersenapi-252628311100% (1)
- Sudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDocument64 pagesSudden Sensorineural Hearing Loss: Christopher D. Muller, M.D. Jeffrey Vrabec, M.DDrKunal KaradeNo ratings yet
- Acute Appendicitis in Pediatric PatientsDocument16 pagesAcute Appendicitis in Pediatric PatientsIgnatius Rheza SetiawanNo ratings yet
- Anatomy Review RespiratoryDocument8 pagesAnatomy Review RespiratoryHanami AsriNo ratings yet
- NCP Ineffective Airway ClearanceDocument5 pagesNCP Ineffective Airway ClearanceEmm Estipona HaoNo ratings yet
- Newborn Care Free Online EditionDocument452 pagesNewborn Care Free Online EditionMayeso E. ChikwalikwaliNo ratings yet
- Humidification in The Intensive Care UnitDocument272 pagesHumidification in The Intensive Care UnitAbu HibbaanNo ratings yet
- LaryngospasmDocument5 pagesLaryngospasmnunikdwijatiNo ratings yet
- Laryngospasm AnesthesiaDocument5 pagesLaryngospasm AnesthesiaLourdes CastilloNo ratings yet
- Anesthesia Considerations in Microlaryngoscopy or Direct LaryngosDocument6 pagesAnesthesia Considerations in Microlaryngoscopy or Direct LaryngosRubén Darío HerediaNo ratings yet
- Bronchospasm During Anaesthesia Update 2011Document5 pagesBronchospasm During Anaesthesia Update 2011hy3pjb1984No ratings yet
- Anaesthesia For Infants and ChildrenDocument9 pagesAnaesthesia For Infants and Childrenapi-142637023No ratings yet
- Anesthesia For Transsphenoidal Pituitary Surgery.Document6 pagesAnesthesia For Transsphenoidal Pituitary Surgery.ismaelNo ratings yet
- A Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionDocument6 pagesA Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionInternational Organization of Scientific Research (IOSR)No ratings yet
- Complicated AppendicitisDocument4 pagesComplicated AppendicitisMedardo ApoloNo ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet
- Post Op LaryngospasmDocument2 pagesPost Op Laryngospasmbalab2311No ratings yet
- Anesthesia For Tracheoesophageal Fistula RepairDocument29 pagesAnesthesia For Tracheoesophageal Fistula RepairArop AkechNo ratings yet
- Perioperative Fluid Management in Pediatrics: By: Karim Kamal, MDDocument33 pagesPerioperative Fluid Management in Pediatrics: By: Karim Kamal, MDMohammed AKNo ratings yet
- 029 Reddy PDFDocument59 pages029 Reddy PDFKonas Xi PalembangNo ratings yet
- Cant Intubate Cant VentilateDocument6 pagesCant Intubate Cant Ventilatedannyromero2712No ratings yet
- Airway ManagementDocument63 pagesAirway ManagementGilang GumilangNo ratings yet
- Stages of AnesthesiaDocument8 pagesStages of Anesthesiajanikka100% (1)
- Diaphragm AnatomyDocument19 pagesDiaphragm AnatomyasujithdrNo ratings yet
- Dexmedetomidine As An Adjuvant To Lignocaine in Intravenous Regional AnesthesiaDocument88 pagesDexmedetomidine As An Adjuvant To Lignocaine in Intravenous Regional AnesthesiaJacob OrtizNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Anaesthesia AIRWAYS, LARYNGOSCOPES, NRVS AND CONNECTORSDocument41 pagesAnaesthesia AIRWAYS, LARYNGOSCOPES, NRVS AND CONNECTORSabciximab100% (2)
- Uptake and Distribution of Volatile AnestheticsDocument22 pagesUptake and Distribution of Volatile AnestheticsSuresh Kumar100% (3)
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- Approach To BreathlessnessDocument5 pagesApproach To BreathlessnessEdy GunawanNo ratings yet
- Anaesthesia in Ophthalmology 001Document37 pagesAnaesthesia in Ophthalmology 001pranab2506No ratings yet
- Acute Exacerbation of Copd & Status AsthmaticusDocument59 pagesAcute Exacerbation of Copd & Status AsthmaticusSaras SinghNo ratings yet
- Otolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Document4 pagesOtolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Adhelline RansunNo ratings yet
- Air Leak SyndromesDocument2 pagesAir Leak SyndromesIchalAzNo ratings yet
- 2013 ASA Guidelines Difficult AirwayDocument20 pages2013 ASA Guidelines Difficult AirwayStacey WoodsNo ratings yet
- Malignant Hyperthermia: Barbara Robertson, MD, FRCPC Dept of Anesthesia, PAHDocument34 pagesMalignant Hyperthermia: Barbara Robertson, MD, FRCPC Dept of Anesthesia, PAHLee Chee SengNo ratings yet
- LaryngospasmDocument3 pagesLaryngospasmbalab2311No ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Bronchiectasis: Dr.K.M.LakshmanarajanDocument238 pagesBronchiectasis: Dr.K.M.LakshmanarajanKM Lakshmana Rajan0% (1)
- 183 Difficult Airway Management (Gabungan)Document135 pages183 Difficult Airway Management (Gabungan)lathifa_nurNo ratings yet
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Evaluation of Dyspneic PatientDocument15 pagesEvaluation of Dyspneic Patientcamila perillaNo ratings yet
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- Bronchial AsthmaDocument25 pagesBronchial AsthmaKamil HannaNo ratings yet
- Surgical Cricothyrotomy (Assist)Document5 pagesSurgical Cricothyrotomy (Assist)ydtrgnNo ratings yet
- Foreign Body AspirationDocument3 pagesForeign Body AspirationAsiya ZaidiNo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Epidural Anatomy & PhysiologyDocument14 pagesEpidural Anatomy & PhysiologyAbel AxelNo ratings yet
- Causes Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As AnDocument22 pagesCauses Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As Anmhelandie100% (1)
- Intravenous Regonal Anaesthesia Biers BlockDocument2 pagesIntravenous Regonal Anaesthesia Biers BlockOkenabirhieNo ratings yet
- 117 - Perioperative HypothermiaDocument4 pages117 - Perioperative HypothermiaYee YeowNo ratings yet
- Adult Chemotherapy Induced Anaphylaxis PolicyDocument12 pagesAdult Chemotherapy Induced Anaphylaxis PolicyMohammed Gazo100% (1)
- Major Haemorrhage ProtocolsDocument3 pagesMajor Haemorrhage ProtocolsleicesterbugNo ratings yet
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocument2 pagesAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- Severe Dengue in ICUDocument35 pagesSevere Dengue in ICUanaeshklNo ratings yet
- Massive TransfusionDocument104 pagesMassive Transfusionbingkydoodle1012No ratings yet
- Regional AnesthesiaDocument54 pagesRegional AnesthesiaIdza Fariha AfriNo ratings yet
- Anesthetic Management of Patients With Major Burn InjuryDocument10 pagesAnesthetic Management of Patients With Major Burn InjuryPablo Eduardo AmadorNo ratings yet
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentFrom EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- Child-Pugh Score: Patient Name: - DateDocument3 pagesChild-Pugh Score: Patient Name: - DateGede Eka Putra NugrahaNo ratings yet
- Intraoperative Recruitment Manoeuvres: Protective Ventilation in The ORDocument7 pagesIntraoperative Recruitment Manoeuvres: Protective Ventilation in The ORGede Eka Putra NugrahaNo ratings yet
- Hazards of Endotracheal AnaesthesiaDocument12 pagesHazards of Endotracheal AnaesthesiaGede Eka Putra NugrahaNo ratings yet
- Psoriasis - Pathophysiology, Conventional, and Alternative Approaches To TreatmentDocument24 pagesPsoriasis - Pathophysiology, Conventional, and Alternative Approaches To TreatmentGede Eka Putra NugrahaNo ratings yet
- Kesehatan Anak Slide Acute Renal FailureDocument21 pagesKesehatan Anak Slide Acute Renal FailureBasory Ok OkNo ratings yet
- Pathogenesis TBDocument39 pagesPathogenesis TBGede Eka Putra NugrahaNo ratings yet
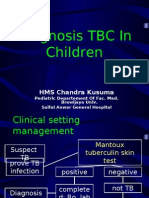
- Diagnosis TBDocument44 pagesDiagnosis TBGede Eka Putra NugrahaNo ratings yet
- Acute Bronchitis: HMS Chandra KusumaDocument16 pagesAcute Bronchitis: HMS Chandra KusumaGede Eka Putra NugrahaNo ratings yet
- Principles of Pulmonary Medicine Eighth Edition Steven E Weinberger Barbara A Cockrill Jess Mandel Online Ebook Texxtbook Full Chapter PDFDocument69 pagesPrinciples of Pulmonary Medicine Eighth Edition Steven E Weinberger Barbara A Cockrill Jess Mandel Online Ebook Texxtbook Full Chapter PDFshayla.broadway739100% (7)
- Findings in Respi. AssessmentDocument13 pagesFindings in Respi. AssessmentChristine LeeNo ratings yet
- AKI CASE NishaDocument64 pagesAKI CASE NishaSurkhali Bipana100% (1)
- Bronchopleural Fistula 1frankDocument105 pagesBronchopleural Fistula 1frankroshjamesNo ratings yet
- ALCOTEC (MSDS) GTAW-ALUMINUM WELD WIRE 7994-N Expires 17-05-01Document9 pagesALCOTEC (MSDS) GTAW-ALUMINUM WELD WIRE 7994-N Expires 17-05-01PubcrawlNo ratings yet
- Objective Test - 1: TOPIC: 1. Respiratory System 2. Circulatory System MM:50Document6 pagesObjective Test - 1: TOPIC: 1. Respiratory System 2. Circulatory System MM:50Jaskirat SinghNo ratings yet
- First Quarterly AssesmentDocument5 pagesFirst Quarterly AssesmentRoana Marie TapiaNo ratings yet
- Breathing and Gas ExchangeDocument8 pagesBreathing and Gas ExchangeSumaiya AnwarNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- NCM 112: (Surgery, CD, I&I, Cellular Aberration) : Lung Cancer (Document8 pagesNCM 112: (Surgery, CD, I&I, Cellular Aberration) : Lung Cancer (Jamaicah N. NagaNo ratings yet
- June Nle 2009 SRG Final CoachingDocument31 pagesJune Nle 2009 SRG Final CoachingChoki Momoki100% (1)
- AsdasdDocument15 pagesAsdasdJohn Paulo RamosNo ratings yet
- Anatomy and Physiology of The Respiratory TractDocument49 pagesAnatomy and Physiology of The Respiratory TractshvnagaNo ratings yet
- 1ST Exam 9-10Document8 pages1ST Exam 9-10Joanne GodezanoNo ratings yet
- SCIENCE 9 Q1-WK 1-2.a FOR STUDENTDocument14 pagesSCIENCE 9 Q1-WK 1-2.a FOR STUDENTErra PeñafloridaNo ratings yet
- BronchiectasisDocument20 pagesBronchiectasisOeyi Mutia SatifaNo ratings yet
- BronchiolitisDocument17 pagesBronchiolitisRizky DarmawanNo ratings yet
- COPD Case Presentation 1Document19 pagesCOPD Case Presentation 1Praveena Mogan100% (1)
- General Biology 2Document22 pagesGeneral Biology 2Lala ChanNo ratings yet
- Nursing Care Plan For Pneumonia NCPDocument2 pagesNursing Care Plan For Pneumonia NCPRoger Jr PumarenNo ratings yet
- Bio4 5Document11 pagesBio4 5HarmonyChuiNo ratings yet
- Science: Quarter 1 - Module 1: Week 1-2Document31 pagesScience: Quarter 1 - Module 1: Week 1-2Kirt Dimamay HilarioNo ratings yet
- Anatomy Lec 13 (Lungs)Document28 pagesAnatomy Lec 13 (Lungs)afzal sulemaniNo ratings yet
- Respiratory Physiology PDFDocument4 pagesRespiratory Physiology PDFDiego AristizabalNo ratings yet