You might also like
- Performance of A Small Scale Haber ProcessDocument9 pagesPerformance of A Small Scale Haber ProcessGuilherme SouzaNo ratings yet
- Hard Gainer - Issue 61 - July 1999Document50 pagesHard Gainer - Issue 61 - July 1999api-3701884100% (7)
- Endolift 980nm+1470nmDocument10 pagesEndolift 980nm+1470nmImran Adeel100% (4)
- NCP For CHDDocument2 pagesNCP For CHDMonica Rivera100% (1)
- Subjective: Sto: DX: DX: STO: Goal MetDocument3 pagesSubjective: Sto: DX: DX: STO: Goal MetFaith BugtongNo ratings yet
- Case Presentation DVTDocument26 pagesCase Presentation DVTimad mokalledNo ratings yet
- Design and Fabrication of Power Scissor JackDocument39 pagesDesign and Fabrication of Power Scissor Jackmohamedovic100% (4)
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
- How To Perform Criticality Analysis To Prioritize Asset MaintenanceDocument22 pagesHow To Perform Criticality Analysis To Prioritize Asset MaintenanceSreekanthMylavarapuNo ratings yet
- NCP Activity IntoleranceDocument2 pagesNCP Activity IntoleranceAce Dioso TubascoNo ratings yet
- NCP For Impaired Physical MobilityDocument2 pagesNCP For Impaired Physical MobilityPrincess Averin Navarro50% (2)
- Practical Cardiovascular PDFDocument462 pagesPractical Cardiovascular PDFbunawanNo ratings yet
- Nursing Care Plan FibromyalgiaDocument2 pagesNursing Care Plan Fibromyalgiaderic90% (10)
- Angeles University Foundation: College of Nursing Nursing Care PlanDocument2 pagesAngeles University Foundation: College of Nursing Nursing Care PlanJohn Cuenco100% (5)
- NCP 5 Ovarian CancerDocument6 pagesNCP 5 Ovarian Cancersaint_ronald886% (29)
- MAHILOM NCP Risk For FallDocument2 pagesMAHILOM NCP Risk For Fallkasandra dawn BerisoNo ratings yet
- NCP GbsDocument2 pagesNCP GbsChristine Lebico100% (2)
- NCP For Aspiration PnuemoniaDocument11 pagesNCP For Aspiration PnuemoniaChristy Rose AgrisNo ratings yet
- Nursing Care Plan For Pregnant Client (Fatigue)Document3 pagesNursing Care Plan For Pregnant Client (Fatigue)Reno Jun Nagasan50% (2)
- Accurately Measure The Patient's Weight and Height. For Baseline DataDocument2 pagesAccurately Measure The Patient's Weight and Height. For Baseline DataMonica RiveraNo ratings yet
- Activity IntoleranceDocument2 pagesActivity IntoleranceMaze Reyes40% (5)
- Subjective Data: Short Term Goal: Short Term GoalDocument3 pagesSubjective Data: Short Term Goal: Short Term GoalNicholas TagleNo ratings yet
- NCP For Impaired Physical MobilityDocument2 pagesNCP For Impaired Physical MobilityPrincess Averin NavarroNo ratings yet
- NURSING CARE PLAN - SuicidalactDocument4 pagesNURSING CARE PLAN - SuicidalactJennifer ArdeNo ratings yet
- Myasthenia Gravis NCPDocument1 pageMyasthenia Gravis NCPCzarina0% (1)
- 3 NCP AsthmaDocument6 pages3 NCP AsthmajaninenicoleNo ratings yet
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- CASEDocument2 pagesCASEBtob melo100% (1)
- Angeles University Foundation: College of Nursing Nursing Care PlanDocument2 pagesAngeles University Foundation: College of Nursing Nursing Care PlanJohn CuencoNo ratings yet
- Nursing Care PlanDocument18 pagesNursing Care PlanElla Grace PradoNo ratings yet
- Assessment Diagnosis Planning Implementatio N Evaluation: Subjective: Short Term: Short TermDocument2 pagesAssessment Diagnosis Planning Implementatio N Evaluation: Subjective: Short Term: Short TermMaverick LimNo ratings yet
- MAHILOM NCP Impaired Physical MobilityDocument2 pagesMAHILOM NCP Impaired Physical Mobilitykasandra dawn BerisoNo ratings yet
- FHP & NCP - FractureDocument14 pagesFHP & NCP - FractureFrancis AdrianNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportDocument3 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportSergi Lee OrateNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective CuesDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Scientific Explanation Planning Implementation Scientific Rationale Evaluation Subjective Cues24 PAULINO ALDRIN MUJARNo ratings yet
- NCP FormDocument3 pagesNCP FormJasmine diokNo ratings yet
- Bulacan State University College of Nursing City of Malolos, BulacanDocument2 pagesBulacan State University College of Nursing City of Malolos, BulacanMia PascualNo ratings yet
- NCP Severe HypocalcemiaDocument4 pagesNCP Severe HypocalcemiaMark Zedrix MediarioNo ratings yet
- Dementia NCPDocument2 pagesDementia NCPkaloydiaz09No ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: IndependentDocument3 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective: IndependentAce Khiel PeraltaNo ratings yet
- HOPEallgoodsDocument4 pagesHOPEallgoodsMarcJohannes MendozaNo ratings yet
- Nursing Care Plan Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationRenie SerranoNo ratings yet
- NCP VergelDocument3 pagesNCP VergelKelly Vergel de DiosNo ratings yet
- Nursing Care Plan (Surgical, Indiv Patient)Document3 pagesNursing Care Plan (Surgical, Indiv Patient)Nursing LectureNo ratings yet
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Geria NCP, Dela CruzDocument7 pagesGeria NCP, Dela CruzStephany Dela CruzNo ratings yet
- NCPDocument4 pagesNCPJhuRise Ann ManganaNo ratings yet
- Nursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationDocument1 pageNursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationJaylord Verazon100% (1)
- Viii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesViii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale Evaluationhehehe29No ratings yet
- NCP High RiskDocument3 pagesNCP High RiskJanelle Gift SenarloNo ratings yet
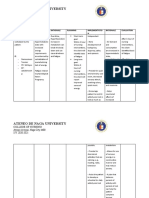
- Ateneo de Naga University: College of NursingDocument4 pagesAteneo de Naga University: College of NursingRenie SerranoNo ratings yet
- NCP StrokeDocument6 pagesNCP StrokeIrish TatelNo ratings yet
- MoblityDocument2 pagesMoblityReyes MikkoNo ratings yet
- Nursing Care Plan For Ischemic Stroke ProblemDocument2 pagesNursing Care Plan For Ischemic Stroke ProblemA HNo ratings yet
- Nursing Care Plan MED SURG NUCDocument4 pagesNursing Care Plan MED SURG NUCRawan KhateebNo ratings yet
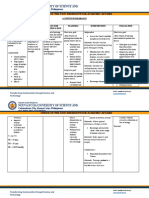
- Nueva Ecija University of Science And: O V A ADocument2 pagesNueva Ecija University of Science And: O V A AVanessa VillanuevaNo ratings yet
- Nag Lilinis NG Sugat Ko, Hindi Ko Kasi Kaya. Mahina Kasi Kalahati NG Katawan Ko" AsDocument4 pagesNag Lilinis NG Sugat Ko, Hindi Ko Kasi Kaya. Mahina Kasi Kalahati NG Katawan Ko" AsNursing LectureNo ratings yet
- NCPDocument6 pagesNCPNik Rose ElNo ratings yet
- PEH NotesDocument1 pagePEH NotesAlyssa Jana Meneses TonogbanuaNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanBelleNo ratings yet
- NCP FatigueDocument2 pagesNCP FatigueKrishna Faith P. DelaraNo ratings yet
- Rabanal, Lovely Jane A. Bsn-Ii Benner MCN Final Exam Case 2Document3 pagesRabanal, Lovely Jane A. Bsn-Ii Benner MCN Final Exam Case 2mark OrpillaNo ratings yet
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- NCP Kuya TedDocument3 pagesNCP Kuya TedBenjie DimayacyacNo ratings yet
- NCPDocument4 pagesNCPmellaNo ratings yet
- NCP PyeloDocument2 pagesNCP PyeloAubrey Unique EvangelistaNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- Mastering Flexibility With Scientific Protocols - Based On The Teachings Of Dr. Andrew Huberman: Optimize Flexibility Using Evidence-Backed Stretching TechniquesFrom EverandMastering Flexibility With Scientific Protocols - Based On The Teachings Of Dr. Andrew Huberman: Optimize Flexibility Using Evidence-Backed Stretching TechniquesNo ratings yet
- Nursing Care Plan For A Person With Croup Nursing DiagnosisDocument2 pagesNursing Care Plan For A Person With Croup Nursing DiagnosisMonica RiveraNo ratings yet
- NCP Post PartumDocument1 pageNCP Post PartumMonica RiveraNo ratings yet
- Nursing Care Plan For A Person With Croup Nursing DiagnosisDocument2 pagesNursing Care Plan For A Person With Croup Nursing DiagnosisMonica Rivera100% (1)
- Almasol 2002 LEDocument2 pagesAlmasol 2002 LEUdit JainNo ratings yet
- Theory of AltruismDocument12 pagesTheory of AltruismPiedra GarcíaNo ratings yet
- Group 19Document24 pagesGroup 19abhishek kumarNo ratings yet
- GRH D 16 00001 ManuscriptDocument224 pagesGRH D 16 00001 ManuscriptsrividyargNo ratings yet
- Hypokalemic Periodic ParalysisDocument5 pagesHypokalemic Periodic ParalysisyanamatshahNo ratings yet
- Occlusal Adjustment For Treating and Preventing Temporomandibular Joint DisordersDocument22 pagesOcclusal Adjustment For Treating and Preventing Temporomandibular Joint DisordersUrsula ValentinaNo ratings yet
- Asian Fit CB Eyewear RangeDocument8 pagesAsian Fit CB Eyewear RangeTan Guat Theng .AshleyNo ratings yet
- Henson, 2001Document24 pagesHenson, 2001maciel27No ratings yet
- Salaries & Wages - Regular Payroll PERA . Due To BIRDocument7 pagesSalaries & Wages - Regular Payroll PERA . Due To BIRAyie RomeroNo ratings yet
- KrylovaDocument515 pagesKrylovaУмер ХудхурNo ratings yet
- Materi WS EWS 2018 - Dr. Dedi - PEWS MEWS OBSEWSDocument59 pagesMateri WS EWS 2018 - Dr. Dedi - PEWS MEWS OBSEWSIndrati TRNo ratings yet
- Ians Pizza Madison MenuDocument4 pagesIans Pizza Madison Menusupport_local_flavorNo ratings yet
- Reoxreaction Quick Revision - 2022Document9 pagesReoxreaction Quick Revision - 2022Hamad FarooqueNo ratings yet
- The Following Text and Tasks Below Ead R Following Text and Tasks Below: The ReadDocument2 pagesThe Following Text and Tasks Below Ead R Following Text and Tasks Below: The Readali ahmadNo ratings yet
- Q.P. Code: 306001 Reg. No.: Third Professional MBBS (Part II) Degree Regular/Supplementary Examinations May 2021 General Medicine - IIDocument1 pageQ.P. Code: 306001 Reg. No.: Third Professional MBBS (Part II) Degree Regular/Supplementary Examinations May 2021 General Medicine - IIJayagovind T JNo ratings yet
- Name: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaDocument3 pagesName: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaMae Therese B. MAGNONo ratings yet
- Activity 1 Rizal Gomburza ExcerptDocument2 pagesActivity 1 Rizal Gomburza ExcerptHyacinth GulbenNo ratings yet
- DV 306 Private Open Space and Communal Open SpaceDocument2 pagesDV 306 Private Open Space and Communal Open SpaceCông QuènNo ratings yet
- Gynea & Obs 26-30Document6 pagesGynea & Obs 26-30Wafiyah AwaisNo ratings yet
- COLD GALVANISING Spray - GBDocument2 pagesCOLD GALVANISING Spray - GBANIL PLAMOOTTILNo ratings yet
- Lenigrad 4 Light Meter PDFDocument9 pagesLenigrad 4 Light Meter PDFRaghul HitmanNo ratings yet
- Cost of Living TORONTODocument1 pageCost of Living TORONTOKasturi JadhavNo ratings yet
- Manual For Quality Seed Production in Wheat.: January 2014Document74 pagesManual For Quality Seed Production in Wheat.: January 2014astuteNo ratings yet