You might also like
- Biostatistician - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandBiostatistician - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Cognitive Function Following Breast Cancer TreatmentDocument4 pagesCognitive Function Following Breast Cancer TreatmentFrancisco MartinezNo ratings yet
- A Study On Health Seeking Behavior Among Married Reproductive Age Group Women in A Rural AreaDocument4 pagesA Study On Health Seeking Behavior Among Married Reproductive Age Group Women in A Rural AreasupriaprNo ratings yet
- Abstract 1 Barriers To Post Surgical Biologic TherDocument2 pagesAbstract 1 Barriers To Post Surgical Biologic Therps piasNo ratings yet
- Low Rate of Dermatology Outpatient Visits in Asian-Americans: An Initial Survey Study For Associated Patient-Related FactorsDocument7 pagesLow Rate of Dermatology Outpatient Visits in Asian-Americans: An Initial Survey Study For Associated Patient-Related FactorsjukilokiNo ratings yet
- Stroke Among Cancer Patients: ArticleDocument8 pagesStroke Among Cancer Patients: Articlevinit sharmaNo ratings yet
- Faktor Risiko Hemoroid Korea NatureDocument9 pagesFaktor Risiko Hemoroid Korea NatureRatu AstridNo ratings yet
- The Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorDocument6 pagesThe Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorIJPHSNo ratings yet
- Medication Errors, P.reddy, Mallesh.Document9 pagesMedication Errors, P.reddy, Mallesh.gnaneshwerNo ratings yet
- 2016 - Ing Ref NoDocument6 pages2016 - Ing Ref NoEstreLLA ValenciaNo ratings yet
- Level of Knowledge of Women Involvement in Voluntary Medical Male Circumcision in Maziba Sub-County Ndorwa East, Kabale DistrictDocument6 pagesLevel of Knowledge of Women Involvement in Voluntary Medical Male Circumcision in Maziba Sub-County Ndorwa East, Kabale DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Incidence and Correlates of Severe Depression and Stigmatization Among HIV Positive Patients Seeking Care at Soroti Regional Referral HospitalDocument13 pagesIncidence and Correlates of Severe Depression and Stigmatization Among HIV Positive Patients Seeking Care at Soroti Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Jama Quinn 2020 Oi 200087 1602283774.26341Document12 pagesJama Quinn 2020 Oi 200087 1602283774.26341charmyshkuNo ratings yet
- Falls in The Elderly - SazlinaDocument6 pagesFalls in The Elderly - SazlinaKrishnanNo ratings yet
- 2 3 1646731639 3ijcnwmcjun20223Document12 pages2 3 1646731639 3ijcnwmcjun20223TJPRC PublicationsNo ratings yet
- Sex Transm Infect. 2011 Aug 87 (5) 385-8Document6 pagesSex Transm Infect. 2011 Aug 87 (5) 385-8Cynthia Patricia Manotas AltamarNo ratings yet
- BayyapareddyDocument8 pagesBayyapareddyeditorijmrhsNo ratings yet
- CPR JournalDocument9 pagesCPR JournalDale DeocaresNo ratings yet
- C. Proposal 1. Overall Goal & ObjectivesDocument13 pagesC. Proposal 1. Overall Goal & ObjectivesDakuro A EthanNo ratings yet
- Regis Class of 2009 AOP ComorbiditiesDocument24 pagesRegis Class of 2009 AOP ComorbiditiesTim Noteboom100% (1)
- Gracelyn Surma: Feasibility and Preliminary Outcomes of An Exercise Intervention in Cancer Survivors: A Pilot StudyDocument24 pagesGracelyn Surma: Feasibility and Preliminary Outcomes of An Exercise Intervention in Cancer Survivors: A Pilot Studyapi-569599709No ratings yet
- BeckDocument6 pagesBeckRenz MacionNo ratings yet
- 22 Ijsrm PDFDocument11 pages22 Ijsrm PDFjaya kumarNo ratings yet
- Khan SlidesDocument17 pagesKhan Slidesalberto cabelloNo ratings yet
- Stress Among Charge NursesDocument10 pagesStress Among Charge NursesRey AllanNo ratings yet
- Prevalence of Diabetes, Associated Symptoms and Risk Factors Among University StudentsDocument8 pagesPrevalence of Diabetes, Associated Symptoms and Risk Factors Among University Studentsijmb333No ratings yet
- B05111723 PDFDocument7 pagesB05111723 PDFdr.owais ahmadNo ratings yet
- Bickel 2018Document6 pagesBickel 2018cpalomero02No ratings yet
- Sociodemographic and Lifestyle Factors As The Risk of Diabetic Foot Ulcer in The University of Malaya Medical CentreDocument7 pagesSociodemographic and Lifestyle Factors As The Risk of Diabetic Foot Ulcer in The University of Malaya Medical Centrelailatul husnaNo ratings yet
- Corona Children Studies Co-Ki First Results of A GDocument15 pagesCorona Children Studies Co-Ki First Results of A GFernando LoaizaNo ratings yet
- The Impact of Depression and Anxiety On The Quality of Life in Nonmetastatic Breast Cancer Patients in Postoperative EvaluationDocument6 pagesThe Impact of Depression and Anxiety On The Quality of Life in Nonmetastatic Breast Cancer Patients in Postoperative EvaluationCamelutza IsaiNo ratings yet
- Hiperbar O2Document22 pagesHiperbar O2Zekany AndreiNo ratings yet
- ENEA PosterDocument6 pagesENEA PosterPrudwiraj SanamandraNo ratings yet
- Healthcare UtilisationDocument4 pagesHealthcare UtilisationIvan RomeroNo ratings yet
- The Open Public Health JournalDocument5 pagesThe Open Public Health JournalSrideviRaviNo ratings yet
- Cushing's DiseaseDocument56 pagesCushing's DiseaseDrasmNo ratings yet
- Community Needs, Concerns, and Perceptions About Health Research - Findings From The Clinical and Translational Science Award Sentinel NetworkDocument8 pagesCommunity Needs, Concerns, and Perceptions About Health Research - Findings From The Clinical and Translational Science Award Sentinel NetworkShera LopezNo ratings yet
- Role of Caregivers' Burden On Qol of DiabeticsDocument17 pagesRole of Caregivers' Burden On Qol of DiabeticsMarufat OdetundeNo ratings yet
- Psoriasis Biologics RegistryDocument6 pagesPsoriasis Biologics RegistryWei Sheng ChongNo ratings yet
- Knowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudyDocument5 pagesKnowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudySrideviRaviNo ratings yet
- Risk Factors For Pelvic Organ Prolapse: C.M. Kim, M.J. Jeon, D.J. Chung, S.K. Kim, J.W. Kim, S.W. BaiDocument4 pagesRisk Factors For Pelvic Organ Prolapse: C.M. Kim, M.J. Jeon, D.J. Chung, S.K. Kim, J.W. Kim, S.W. BaiAkame No IDNo ratings yet
- Risk Factors For 30-Day Readmissions After Acute MDocument7 pagesRisk Factors For 30-Day Readmissions After Acute MFahmi RaziNo ratings yet
- What Is Vaccine Efficacy and Why Is It Important?Document5 pagesWhat Is Vaccine Efficacy and Why Is It Important?Darshan gohilNo ratings yet
- Yates 2017Document13 pagesYates 2017Ambulatório Dieta Cetogênica HUBNo ratings yet
- C. Fullpapper - Manuskrip ICOOPH - Agustus 2022Document13 pagesC. Fullpapper - Manuskrip ICOOPH - Agustus 2022Siti NurjanahNo ratings yet
- Accelerated ART Intro & Research Base Kip PPT 7-19-2017Document44 pagesAccelerated ART Intro & Research Base Kip PPT 7-19-2017scmesser0% (1)
- 1953 PDFDocument4 pages1953 PDFHesti hasanNo ratings yet
- Risk of Falls and Associated Factors Among Older CDocument15 pagesRisk of Falls and Associated Factors Among Older Cmariasol63No ratings yet
- Tumor Characteristics and Their Relationship To Colorectal Cancer RelapseDocument1 pageTumor Characteristics and Their Relationship To Colorectal Cancer RelapsePopa TiberiuNo ratings yet
- Assessment Test. RevisedDocument16 pagesAssessment Test. RevisedBrian KyaloNo ratings yet
- Diagnostic Progression To Bipolar Disorder in 17,285 Adolescents and Young AdultsDocument7 pagesDiagnostic Progression To Bipolar Disorder in 17,285 Adolescents and Young AdultsCarla NapoliNo ratings yet
- Admin,+20+023p+ +revisi+ +Dewi+Indah+Lestari - Edited+173 180Document8 pagesAdmin,+20+023p+ +revisi+ +Dewi+Indah+Lestari - Edited+173 180CerileeNo ratings yet
- A.Baqi Article 2 - RevisedDocument9 pagesA.Baqi Article 2 - RevisedAbdul Baqi KhanNo ratings yet
- Assessment Test. RevisedDocument16 pagesAssessment Test. RevisedBrian KyaloNo ratings yet
- A Study On Hivaids Knowledge Among Nursing StudentDocument6 pagesA Study On Hivaids Knowledge Among Nursing Studentanastasia mumeckhNo ratings yet
- Missing AppointmentsDocument6 pagesMissing Appointmentsaleeza sanaNo ratings yet
- HPV Vaccine 1Document18 pagesHPV Vaccine 1Simran ChauhanNo ratings yet
- Patients Admitted To Tertiary Health Care Center: Cancer Screening Program Awareness StudyDocument3 pagesPatients Admitted To Tertiary Health Care Center: Cancer Screening Program Awareness StudyPeertechz Publications Inc.No ratings yet
- Three Questions To Screen Your Patients For Chemical, Food, and Drug Intolerances The Brief Environmental Exposure and Sensitivity Inventory (Breesi)Document13 pagesThree Questions To Screen Your Patients For Chemical, Food, and Drug Intolerances The Brief Environmental Exposure and Sensitivity Inventory (Breesi)Eman SwaidanNo ratings yet
- Hungarian Outlook - Tax Reduction and Minimum Wage Increase in HungaryDocument4 pagesHungarian Outlook - Tax Reduction and Minimum Wage Increase in HungaryGary LheureuxNo ratings yet
- Cancers 12 03000Document13 pagesCancers 12 03000Gary LheureuxNo ratings yet
- Castrol Alphasyn T46 EnglishDocument15 pagesCastrol Alphasyn T46 EnglishGary LheureuxNo ratings yet
- Din en Iso 4287-2010Document31 pagesDin en Iso 4287-2010Gary LheureuxNo ratings yet
- Din en Iso 4287-2010Document31 pagesDin en Iso 4287-2010Gary LheureuxNo ratings yet
- Castrol Alphasyn T46 EnglishDocument15 pagesCastrol Alphasyn T46 EnglishGary LheureuxNo ratings yet
- Hungarian Outlook - Tax Reduction and Minimum Wage Increase in HungaryDocument4 pagesHungarian Outlook - Tax Reduction and Minimum Wage Increase in HungaryGary LheureuxNo ratings yet
- h1 Styleclearboth Idcontentsection0the Only Guide To Commercial Fisheries Reviewh1jbfch PDFDocument14 pagesh1 Styleclearboth Idcontentsection0the Only Guide To Commercial Fisheries Reviewh1jbfch PDFgalleymark22No ratings yet
- 10th Grade Argumentative RubricDocument1 page10th Grade Argumentative Rubricapi-253371643No ratings yet
- Afa 7&8Document11 pagesAfa 7&8APMNo ratings yet
- Life After Ashes: Understanding The Impact of Business Loss To The Livelihood of San Fernando City Wet Market VendorsDocument10 pagesLife After Ashes: Understanding The Impact of Business Loss To The Livelihood of San Fernando City Wet Market Vendorsalrichj29No ratings yet
- Case StudyDocument11 pagesCase StudyCyril CauilanNo ratings yet
- Presentation by SHIVAM SHAHDocument23 pagesPresentation by SHIVAM SHAHmikojiNo ratings yet
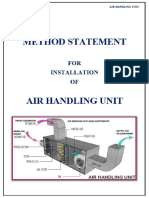
- Method Statement Installation of Air Handling UntDocument6 pagesMethod Statement Installation of Air Handling UntkouarNo ratings yet
- Venkateshetal 2003Document56 pagesVenkateshetal 2003Gilang KemalNo ratings yet
- IHS Markit Seed Market Analysis and Data InfographicDocument1 pageIHS Markit Seed Market Analysis and Data Infographictripurari pandeyNo ratings yet
- Sciencedirect: Development of Battery Monitoring System in Smart Microgrid Based On Internet of Things (Iot)Document6 pagesSciencedirect: Development of Battery Monitoring System in Smart Microgrid Based On Internet of Things (Iot)KiranNo ratings yet
- Product Data Sheet: Product Description Technical SpecificationDocument1 pageProduct Data Sheet: Product Description Technical SpecificationYASHICA VAITTIANATHANNo ratings yet
- Thermodynamics JAM 2021 1Document42 pagesThermodynamics JAM 2021 1krishna prasad ghanta100% (2)
- Review Iftekher 2013Document11 pagesReview Iftekher 2013RezaNo ratings yet
- Philippine Board of Nursing Course SyllabusDocument11 pagesPhilippine Board of Nursing Course SyllabusChin Chan100% (1)
- P, PI and PID ControlDocument3 pagesP, PI and PID ControlsivaNo ratings yet
- Saidin PSC - SHO UTMSPACE - 13.01.22 Module Slide 6s - LDocument43 pagesSaidin PSC - SHO UTMSPACE - 13.01.22 Module Slide 6s - LAmer IkhwanNo ratings yet
- Curriculam Vitae OF MD - Nazmus Sakib Khan: Career ObjectivesDocument4 pagesCurriculam Vitae OF MD - Nazmus Sakib Khan: Career ObjectivesRubayetNo ratings yet
- CRE Chapter 5 (Solutions)Document8 pagesCRE Chapter 5 (Solutions)Bella HannaNo ratings yet
- Classroom of The Elite Vol. 8Document244 pagesClassroom of The Elite Vol. 8Rahul Lakra85% (13)
- Line Scan (Switch Hook) : NamesDocument3 pagesLine Scan (Switch Hook) : NamesUsairumNo ratings yet
- I Learned Chapter 8-The Power of GuidanceDocument1 pageI Learned Chapter 8-The Power of Guidanceapi-295870335No ratings yet
- SM2 Polygon of ForcesDocument11 pagesSM2 Polygon of ForcesMel DNo ratings yet
- Đề Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Document8 pagesĐề Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Chi Vũ LinhNo ratings yet
- Proton-Halo Breakup DynamicsDocument7 pagesProton-Halo Breakup DynamicsBharat KashyapNo ratings yet
- A Summary of The Theories or Concepts About Child Development From Piaget, Vygotsky, Brunner, and Gardner-Zahra Warda Mufidah 183221217Document16 pagesA Summary of The Theories or Concepts About Child Development From Piaget, Vygotsky, Brunner, and Gardner-Zahra Warda Mufidah 183221217Fida100% (1)
- Contact Inform 2002 OldDocument22 pagesContact Inform 2002 OldBelajar PurboNo ratings yet
- Scaffold 2Document3 pagesScaffold 2Mahmoud Elsayed MohamedNo ratings yet
- One-Dimensional Unconstrained Optimization: Example 1 Golden Section MethodDocument5 pagesOne-Dimensional Unconstrained Optimization: Example 1 Golden Section MethodMohamed MuayidNo ratings yet
- 6480 49 35800 2 10 20230801Document12 pages6480 49 35800 2 10 20230801samsidar nidarNo ratings yet
- IE54500 - Exam 1: Dr. David Johnson Fall 2020Document7 pagesIE54500 - Exam 1: Dr. David Johnson Fall 2020MNo ratings yet