You might also like
- 2022 Clinthera S1T4 Copd PDFDocument5 pages2022 Clinthera S1T4 Copd PDFmedicoNo ratings yet
- First AidDocument32 pagesFirst Aidnikolas.elias22No ratings yet
- Artemisia Absinthium, Linn. Common Wormwood. (Europe.) Not To Be Confounded With Artemisia Vulgaris, Which Is Also Called Wormwood. N. O. Compositæ. Tincture of Fresh Young Leaves and FlowersDocument3 pagesArtemisia Absinthium, Linn. Common Wormwood. (Europe.) Not To Be Confounded With Artemisia Vulgaris, Which Is Also Called Wormwood. N. O. Compositæ. Tincture of Fresh Young Leaves and FlowersKamalNo ratings yet
- Acid Base ABG’s and Electrolytes ExplainedDocument25 pagesAcid Base ABG’s and Electrolytes ExplainedMelissa Sapp96% (28)
- CHF NewDocument7 pagesCHF NewJyoti SidhuNo ratings yet
- Cardiology: C B: A V L U: J 2019Document20 pagesCardiology: C B: A V L U: J 2019Owen AgnewNo ratings yet
- Cardiology HX - PEDocument34 pagesCardiology HX - PEjjNo ratings yet
- Cardiovascular System: A Comprehensive Review of Presenting SymptomsDocument38 pagesCardiovascular System: A Comprehensive Review of Presenting SymptomsChethranNo ratings yet
- Respiratory ENT Assessment GuideDocument3 pagesRespiratory ENT Assessment GuidepriyaNo ratings yet
- Koma dan Penurunan KesadaranDocument40 pagesKoma dan Penurunan KesadaranAhmad Shafwan NatsirNo ratings yet
- RespiratoryDocument7 pagesRespiratoryThomas KearneyNo ratings yet
- Mrs. Hernandez Shortness of BreathDocument7 pagesMrs. Hernandez Shortness of BreathChananNo ratings yet
- Taller Enfermedades GaboDocument6 pagesTaller Enfermedades GaboAndy RamirezNo ratings yet
- Rad 2119 First Aid 3Document27 pagesRad 2119 First Aid 3Casper ScholesNo ratings yet
- Kent - NajaDocument3 pagesKent - Najaaldodias100% (1)
- CPRDocument27 pagesCPRfaizuraNo ratings yet
- DYSPNOEADocument19 pagesDYSPNOEAvedha mungaraNo ratings yet
- First Aid Glossary - 40 Essential Terms ExplainedDocument12 pagesFirst Aid Glossary - 40 Essential Terms ExplainedMohamed AbdiNo ratings yet
- A.Chest Wall Abnormalities: 1.) Respiratory SystemDocument6 pagesA.Chest Wall Abnormalities: 1.) Respiratory SystemAlhadzra AlihNo ratings yet
- OSCE Chart Cough (KK)Document4 pagesOSCE Chart Cough (KK)api-26938624No ratings yet
- Assessing Heart and Neck VesselsDocument7 pagesAssessing Heart and Neck VesselsJae TyNo ratings yet
- DRRRRRRRDocument5 pagesDRRRRRRRtocoj18582No ratings yet
- FirstAid SlidesDocument62 pagesFirstAid Slidessamihamaideh100% (1)
- BPPV Diagnosis and TreatmentDocument9 pagesBPPV Diagnosis and TreatmentKristanne Louise YuNo ratings yet
- Clinical Pharmacy NotesDocument3 pagesClinical Pharmacy NotesMary Charmaine DivinagraciaNo ratings yet
- Peros: General AssessmentDocument4 pagesPeros: General AssessmentKaycee TolingNo ratings yet
- The Nervous SystemDocument24 pagesThe Nervous SystemKiara GovenderNo ratings yet
- Respiratory Examination - Protected 1Document4 pagesRespiratory Examination - Protected 1anirudh811100% (1)
- Compilation of MS NotesDocument81 pagesCompilation of MS Notesdis_is_meNo ratings yet
- Vomiting of Gastrointestinal OriginDocument4 pagesVomiting of Gastrointestinal OriginFathimathNo ratings yet
- Asphyxia and BarotraumaDocument10 pagesAsphyxia and BarotraumadeevoncNo ratings yet
- Essential Basics of General Medicine Faculty of Dentistry Cairo UniversityDocument104 pagesEssential Basics of General Medicine Faculty of Dentistry Cairo Universitybavly waidyNo ratings yet
- Diagnosis of Dyspnea 2011 VTDocument77 pagesDiagnosis of Dyspnea 2011 VTRovanNo ratings yet
- Hypernatremia Hyperkalemia: of Increased Serum K+Document3 pagesHypernatremia Hyperkalemia: of Increased Serum K+edited_chenNo ratings yet
- Common homeopathic remedies for heart diseaseDocument9 pagesCommon homeopathic remedies for heart diseasessNo ratings yet
- Bay Area College of Nursing: Module 12: Emergency ProcedureDocument6 pagesBay Area College of Nursing: Module 12: Emergency Procedurepilsen_01No ratings yet
- anapiDocument4 pagesanapianastaziaarcayeraNo ratings yet
- Caisson's Disease and Nitrogen Bubbles in JointsDocument630 pagesCaisson's Disease and Nitrogen Bubbles in JointsAnurag Behera100% (1)
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 pagesPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Health AssessmentDocument3 pagesHealth AssessmentAndrea Jewel BaladjayNo ratings yet
- Shortness of Breath: ER Perspective Shaesta TabassumDocument46 pagesShortness of Breath: ER Perspective Shaesta TabassumAjay DherwaniNo ratings yet
- MS LEC Reviewer Oxygenation ProblemsDocument8 pagesMS LEC Reviewer Oxygenation ProblemsVinzii DrtNo ratings yet
- StrokeDocument4 pagesStrokeMostafa SaadawyNo ratings yet
- CN 118 - Assessment (Reviewer)Document5 pagesCN 118 - Assessment (Reviewer)Camille SanguyoNo ratings yet
- Draft Sleep ApneaDocument7 pagesDraft Sleep ApneaJul Jainnah G. AdilNo ratings yet
- Assignment 1Document2 pagesAssignment 1Pam ArienzaNo ratings yet
- Head Injuries FAST CheckDocument20 pagesHead Injuries FAST CheckCasper ScholesNo ratings yet
- COPDDocument4 pagesCOPDitsmailbbkNo ratings yet
- Pleural Conditions Arf Ards PeDocument4 pagesPleural Conditions Arf Ards PeNoreen PadillaNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Syncope, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandSyncope, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Epilepsy, Hysteria, and Neurasthenia: Their Causes, Symptoms, & TreatmentFrom EverandEpilepsy, Hysteria, and Neurasthenia: Their Causes, Symptoms, & TreatmentNo ratings yet
- Apnea No More: Easy Ways Out Of Sleep ApneaFrom EverandApnea No More: Easy Ways Out Of Sleep ApneaRating: 5 out of 5 stars5/5 (1)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Subsea Pipeline InspectionDocument41 pagesSubsea Pipeline InspectionMukil Dev100% (3)
- Wis5 Welding Defects 02Document55 pagesWis5 Welding Defects 02Lely Asri100% (1)
- Doing Bus in Gib 2012 13Document132 pagesDoing Bus in Gib 2012 13RicardoNo ratings yet
- Efc Membership Application Form: 0034 679770011 Info@m6subseatraining Ricardo SoaresDocument1 pageEfc Membership Application Form: 0034 679770011 Info@m6subseatraining Ricardo SoaresRicardoNo ratings yet
- English Grammar Guide from Colegio Concertado Ntra. Sra. de la ProvidenciaDocument27 pagesEnglish Grammar Guide from Colegio Concertado Ntra. Sra. de la ProvidenciaJose Andres Martinez Garcia100% (2)
- Dirty Harry': World Leaders in Diving Equipment TechnologyDocument4 pagesDirty Harry': World Leaders in Diving Equipment TechnologyRicardoNo ratings yet
- Inpp Activites 2007Document2 pagesInpp Activites 2007RicardoNo ratings yet
- Living and Working NorwayDocument28 pagesLiving and Working NorwayRicardo100% (1)
- Certification and Training MatrixDocument1 pageCertification and Training MatrixRicardoNo ratings yet
- Hydrex Magazine 207Document16 pagesHydrex Magazine 207RicardoNo ratings yet
- Human Physiology in An Aquatic EnvironmeDocument46 pagesHuman Physiology in An Aquatic EnvironmeRicardoNo ratings yet
- Rubber and HAZTECH Bio ResultsDocument1 pageRubber and HAZTECH Bio ResultsRicardoNo ratings yet
- Argon Radiation Safety Training EbookDocument14 pagesArgon Radiation Safety Training EbookBruno Luis Villarroel DávalosNo ratings yet
- Argon - Improving First Responder Radiation Safety TrainingDocument7 pagesArgon - Improving First Responder Radiation Safety TrainingRicardoNo ratings yet
- M6 Simply Clever: Make Your Job EasierDocument5 pagesM6 Simply Clever: Make Your Job EasierRicardoNo ratings yet
- 1 Alocit-How It Works - UW and WetDocument7 pages1 Alocit-How It Works - UW and WetRicardoNo ratings yet
- Portfolio Guide 2015Document56 pagesPortfolio Guide 2015RicardoNo ratings yet
- Temporarypermanent Pipe Repair - GuidelinesDocument70 pagesTemporarypermanent Pipe Repair - Guidelinesqinaip100% (1)
- M6 Subsea TrainingDocument1 pageM6 Subsea TrainingRicardoNo ratings yet
- M6 Hull Cleaning MachineDocument4 pagesM6 Hull Cleaning MachineRicardoNo ratings yet
- Cut Costs!: A Clean Hull Makes Major SavingsDocument4 pagesCut Costs!: A Clean Hull Makes Major SavingsRicardo100% (1)
- High-Pressure Water Jetting Systems: Stationary and Mobile Systems 25 - 1,000 HPDocument6 pagesHigh-Pressure Water Jetting Systems: Stationary and Mobile Systems 25 - 1,000 HPSamsuNo ratings yet
- I-Tech Services: Delivering Integrated Services and Products Across The Field Life CycleDocument5 pagesI-Tech Services: Delivering Integrated Services and Products Across The Field Life CycleRicardoNo ratings yet
- Infra Estructuras Necesarias para OFFSHOREDocument256 pagesInfra Estructuras Necesarias para OFFSHORERicardoNo ratings yet
- What Determine Investment in Oil Sector PDFDocument49 pagesWhat Determine Investment in Oil Sector PDFBagus Deddy AndriNo ratings yet
- Project: 2007-2008 Biennial Underwater Bridge Location: Syracuse To Buffalo, New York OwnerDocument1 pageProject: 2007-2008 Biennial Underwater Bridge Location: Syracuse To Buffalo, New York OwnerRicardoNo ratings yet
- Estudio de Diferentes Infra Estructuras PortuariaDocument281 pagesEstudio de Diferentes Infra Estructuras PortuariaRicardoNo ratings yet
- Project: 2007-2008 Biennial Underwater Bridge Location: Syracuse To Buffalo, New York OwnerDocument1 pageProject: 2007-2008 Biennial Underwater Bridge Location: Syracuse To Buffalo, New York OwnerRicardoNo ratings yet
- Mitt80001 Part2Document41 pagesMitt80001 Part2RicardoNo ratings yet
- Underwater Bridge Inspection: Publication No. FHWA-NHI-10-027Document224 pagesUnderwater Bridge Inspection: Publication No. FHWA-NHI-10-027RicardoNo ratings yet
- Ss Organ Systems WorksheetDocument2 pagesSs Organ Systems Worksheet땡뿍뿍No ratings yet
- Maria Victoria Hofileña, M.D.: AnesthesiologyDocument6 pagesMaria Victoria Hofileña, M.D.: AnesthesiologyAbegail IbañezNo ratings yet
- Ginhawa Sprint PlanDocument1 pageGinhawa Sprint PlanHAZEL JEAN BIGCASNo ratings yet
- Calibration of Self-Contained Breathing Apparatus: Dr. Nour F. AttiaDocument14 pagesCalibration of Self-Contained Breathing Apparatus: Dr. Nour F. AttiaAhmed AwwadNo ratings yet
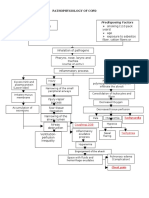
- Pathophysiology of COPDDocument1 pagePathophysiology of COPDDimpal ChoudharyNo ratings yet
- MSDS Wüfoam 70 Megamax Würth (EN)Document19 pagesMSDS Wüfoam 70 Megamax Würth (EN)BradyNo ratings yet
- Abg NursingDocument21 pagesAbg NursingCharisse TaylanNo ratings yet
- Quick Quiz: On Your Answer Sheet, Write in or Circle The Correct Letter For Each QuestionDocument2 pagesQuick Quiz: On Your Answer Sheet, Write in or Circle The Correct Letter For Each QuestionOneth RajapakseNo ratings yet
- Butyl Acrylate MSDSDocument12 pagesButyl Acrylate MSDSMohamed HalemNo ratings yet
- NCP SDocument8 pagesNCP SMarvie CadenaNo ratings yet
- Ayurvedic TreatmentsDocument7 pagesAyurvedic Treatmentsra222j2390% (1)
- Reference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Document3 pagesReference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Kris Marie DelaCruz DomingoNo ratings yet
- Safety Data Sheet: Serological Research Institute (SERI)Document6 pagesSafety Data Sheet: Serological Research Institute (SERI)marthacoolNo ratings yet
- Case Presentation-Neonatal SepsisDocument22 pagesCase Presentation-Neonatal SepsisDianne Dawn0% (1)
- Feasibility of Shared Mechanical Ventilation: Factibilidad de La Ventilación Mecánica CompartidaDocument5 pagesFeasibility of Shared Mechanical Ventilation: Factibilidad de La Ventilación Mecánica CompartidaadnanNo ratings yet
- Test 5 & 6 BDSDocument19 pagesTest 5 & 6 BDSrababNo ratings yet
- Egg Albumin MSDSDocument5 pagesEgg Albumin MSDSFransLei Vadoel SaelNo ratings yet
- Digestive System (Anatomy)Document11 pagesDigestive System (Anatomy)Akash SuryavanshiNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Outpatient Management in Adults - UpToDateDocument29 pagesCoronavirus Disease 2019 (COVID-19) - Outpatient Management in Adults - UpToDateSofia PellecerNo ratings yet
- SDS 791471000 Inconel 718 English EUDocument9 pagesSDS 791471000 Inconel 718 English EUConstantin Romica StoicaNo ratings yet
- Dräger Evita V800 ICU Ventilation and Respiratory MonitoringDocument10 pagesDräger Evita V800 ICU Ventilation and Respiratory MonitoringdawitNo ratings yet
- EnglishDocument3 pagesEnglishAlana MesquitaNo ratings yet
- E000367 FullDocument15 pagesE000367 FullBBD BBDNo ratings yet
- American Academy of PediatricsDocument320 pagesAmerican Academy of PediatricsJuan Sebasatián Arjona100% (2)
- Lalana Newborn ResuscitationDocument55 pagesLalana Newborn ResuscitationAthenaeum Scientific PublishersNo ratings yet
- Care Planning for BreathlessnessDocument14 pagesCare Planning for BreathlessnesspriscellaNo ratings yet
- Health Week 1-3 - 3rd QuarterDocument8 pagesHealth Week 1-3 - 3rd QuarterNoemelyn VecinaNo ratings yet
- K0K ( - 8 - 85 - 2 - PDFDocument162 pagesK0K ( - 8 - 85 - 2 - PDFCecilia LecuvaNo ratings yet
- NGNTestPacket 110322Document64 pagesNGNTestPacket 110322romeliza romeliza0% (1)
- RT0915t10 - Splbe Top 10Document1 pageRT0915t10 - Splbe Top 10Angela JuliaNo ratings yet