You might also like
- ONSITE Resources: Total Project CostDocument3 pagesONSITE Resources: Total Project Costsunil sakriNo ratings yet
- Fabrication Cost Estimation Including ManpowerDocument33 pagesFabrication Cost Estimation Including ManpowerVinayak PujariNo ratings yet
- Rmdjv-pj74-Hiradc-subc 03 (Hoisting & Rigging)Document1 pageRmdjv-pj74-Hiradc-subc 03 (Hoisting & Rigging)myn maliQueNo ratings yet
- A Commercial General LiabilityDocument2 pagesA Commercial General LiabilityTarannum khatri100% (1)
- CPR/AED/First Aid TrainingDocument50 pagesCPR/AED/First Aid TrainingThe Health Therapist AcademyNo ratings yet
- Man Hour EstimateDocument1 pageMan Hour EstimatemuradagasiyevNo ratings yet
- Cambodian School of Prosthetics and Orthotics: CSPO ManualDocument60 pagesCambodian School of Prosthetics and Orthotics: CSPO ManualBilalNo ratings yet
- Construction Safety Program TemplateDocument15 pagesConstruction Safety Program TemplateSole Kicks PHNo ratings yet
- Midface FracturesDocument31 pagesMidface FracturesJoyabrata SarkarNo ratings yet
- Tower Crane InstallationDocument6 pagesTower Crane InstallationTir Dan Knight100% (5)
- Work Order TemplateDocument2 pagesWork Order TemplateRed DragonNo ratings yet
- Test Bank For Sectional Anatomy For Imaging Professionals 4th Edition by KelleyDocument5 pagesTest Bank For Sectional Anatomy For Imaging Professionals 4th Edition by KelleyDavid Perry100% (31)
- Project Budget PlannerDocument25 pagesProject Budget PlannerHussain ElarabiNo ratings yet
- Emergency and Disaster NursingDocument20 pagesEmergency and Disaster NursingNeil Cuasito89% (9)
- H&S Monthly StatsDocument6 pagesH&S Monthly StatsvarunstuffNo ratings yet
- LPG SafetyDocument28 pagesLPG Safetybenaoumeur benouna0% (1)
- Income Statement V 1 1Document7 pagesIncome Statement V 1 1Akbar AliNo ratings yet
- Villages Water Supply System, Inc.: Project: LocationDocument4 pagesVillages Water Supply System, Inc.: Project: LocationJohnlerie EsguerraNo ratings yet
- Set Full Yem Khau TrangDocument1 pageSet Full Yem Khau TranguyenmoclenNo ratings yet
- Project: Location:: Scope of Work Labor Cost XDocument4 pagesProject: Location:: Scope of Work Labor Cost XJohnlerie EsguerraNo ratings yet
- Anai - AnaiDocument199 pagesAnai - AnaiNizzamGetNo ratings yet
- Re-Roofing and Fencing Calaba, Bangued AbraDocument28 pagesRe-Roofing and Fencing Calaba, Bangued AbraReynoldPacurzaNo ratings yet
- Unit Cost Analysis As of April 2003: Sub Total (Materials)Document42 pagesUnit Cost Analysis As of April 2003: Sub Total (Materials)mymian1315No ratings yet
- A0 Set-Full-Yem-Khau-TrangDocument1 pageA0 Set-Full-Yem-Khau-TranguyenmoclenNo ratings yet
- Villages Water Supply System, Inc.: Project: LocationDocument4 pagesVillages Water Supply System, Inc.: Project: LocationJohnlerie EsguerraNo ratings yet
- Project: Location:: Scope of Work Labor Cost XDocument4 pagesProject: Location:: Scope of Work Labor Cost XJohnlerie EsguerraNo ratings yet
- (SINGLE END) JackingDocument60 pages(SINGLE END) Jackingedc1312No ratings yet
- Payroll Report Template 02 PDF Employment PDocument1 pagePayroll Report Template 02 PDF Employment Pkramergeorgec397No ratings yet
- Payroll Report Template 02Document1 pagePayroll Report Template 02dah viral?No ratings yet
- Pharmacist Grade AssesmentDocument6 pagesPharmacist Grade AssesmentSheik MohammedNo ratings yet
- Job Request Form2Document4 pagesJob Request Form2Johnlerie EsguerraNo ratings yet
- Job Request Form2Document4 pagesJob Request Form2Johnlerie EsguerraNo ratings yet
- Staff Present During The Work: List of Worker Working at NightDocument2 pagesStaff Present During The Work: List of Worker Working at NightVikas YamagarNo ratings yet
- Remember To Save This Worksheet As The Name of Your New TankDocument3 pagesRemember To Save This Worksheet As The Name of Your New TankEsadomesNo ratings yet
- Man Hour EstimateDocument1 pageMan Hour EstimateDAYONo ratings yet
- HDG Tertiary Structure: Daily Progress Report - PT Prospera Brillar IndonesiaDocument3 pagesHDG Tertiary Structure: Daily Progress Report - PT Prospera Brillar IndonesiaTadaya KasaharaNo ratings yet
- Parnika RevisedDocument1 pageParnika Revisedparas INSURANCENo ratings yet
- Contoh Work Order InstructionDocument96 pagesContoh Work Order InstructionMohd Azizi Verminator50% (2)
- (2021-05) Form Ide Absensi Manual Ngawi MayDocument447 pages(2021-05) Form Ide Absensi Manual Ngawi Mayrizki darmawanNo ratings yet
- 6.0 Weekly Health and Safety ReportDocument369 pages6.0 Weekly Health and Safety ReportJoachimNo ratings yet
- Weekly Time SheetDocument1 pageWeekly Time SheetYasin ALAINo ratings yet
- Project: Location:: Scope of Work Labor Cost XDocument4 pagesProject: Location:: Scope of Work Labor Cost XJohnlerie EsguerraNo ratings yet
- Sushant Saurav: Job InformationDocument10 pagesSushant Saurav: Job InformationSushant SauravNo ratings yet
- Grade Sheets 1Document1 pageGrade Sheets 1Arwin John LizardoNo ratings yet
- Analytical Calibration Using A Reversed Cubic Curve FitDocument12 pagesAnalytical Calibration Using A Reversed Cubic Curve FitNoah ZlinNo ratings yet
- Factura Proforma Castellano InglésDocument2 pagesFactura Proforma Castellano InglésANĐERSONNo ratings yet
- Salary Sheet FormatDocument2 pagesSalary Sheet FormatAmir ShaikhNo ratings yet
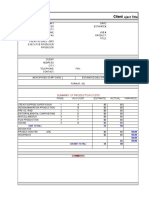
- Client: Oject TitleDocument4 pagesClient: Oject TitlePANo ratings yet
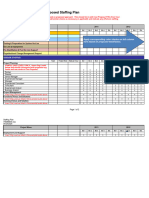
- Staffing Plan Template 31Document2 pagesStaffing Plan Template 31Milin Anik'sNo ratings yet
- Project Budget PlannerDocument42 pagesProject Budget Plannernsadnan100% (2)
- Bill of Material: "Zal"-Denotes " Zincalume"Document10 pagesBill of Material: "Zal"-Denotes " Zincalume"sunil sarafNo ratings yet
- QEC Calculation Tool TemplateDocument7 pagesQEC Calculation Tool Templateruhul bayanNo ratings yet
- 1 Individual: Project at A Glance - Top SheetDocument10 pages1 Individual: Project at A Glance - Top SheetDigital InfotechNo ratings yet
- 05-Understanding RPMS Tools and MOVsDocument6 pages05-Understanding RPMS Tools and MOVsJhemitch Jhea ArtigoNo ratings yet
- Daily Night Work Permission Form: List of Worker Working at NightDocument2 pagesDaily Night Work Permission Form: List of Worker Working at NightVikas YamagarNo ratings yet
- WFP BlankDocument18 pagesWFP BlankJRNo ratings yet
- Daily ReportDocument35 pagesDaily ReportBaba YagaNo ratings yet
- CanopyDocument4 pagesCanopyanonymousupldr666No ratings yet
- Tito LouieDocument92 pagesTito LouieBobby GalvezNo ratings yet
- SegmentDocument117 pagesSegmentAshish KhandekarNo ratings yet
- Daily Report - 05.10.2021Document3 pagesDaily Report - 05.10.2021Shohel RanaNo ratings yet
- Algort Technosolutions NewDocument1 pageAlgort Technosolutions Newparas INSURANCENo ratings yet
- Film Budget Template 01Document12 pagesFilm Budget Template 01Marielle PerejonNo ratings yet
- Fiber Optic Master File Rev 2Document44 pagesFiber Optic Master File Rev 2Mohamed RafihNo ratings yet
- Daily Fuel Expense (Recovered)Document4 pagesDaily Fuel Expense (Recovered)ankit sharmaNo ratings yet
- Attendance Report For Salaried Employees: The University CorporationDocument1 pageAttendance Report For Salaried Employees: The University CorporationimtiazbscNo ratings yet
- Celtx Call Sheet TemplateDocument1 pageCeltx Call Sheet TemplateJean-Louis SénécautNo ratings yet
- Appendix 7. GlossaryDocument1 pageAppendix 7. Glossarybenaoumeur benounaNo ratings yet
- Appendix 5. Risk AnalysisDocument1 pageAppendix 5. Risk Analysisbenaoumeur benounaNo ratings yet
- Your Logo Here: Safe Work Method StatementDocument2 pagesYour Logo Here: Safe Work Method Statementbenaoumeur benounaNo ratings yet
- Review of Tenders Contracts and Projects: Form: 1032Document2 pagesReview of Tenders Contracts and Projects: Form: 1032benaoumeur benounaNo ratings yet
- Appendix 6. Field Visit ReportDocument1 pageAppendix 6. Field Visit Reportbenaoumeur benounaNo ratings yet
- Liquefied Natural Gas - WikipediaDocument1 pageLiquefied Natural Gas - Wikipediabenaoumeur benounaNo ratings yet
- Sunrise LNG - Dreams, Realities and Challenges. AcknowledgementsDocument1 pageSunrise LNG - Dreams, Realities and Challenges. Acknowledgementsbenaoumeur benounaNo ratings yet
- Fire Fighting SystemsDocument61 pagesFire Fighting Systemsbenaoumeur benounaNo ratings yet
- FMEA Form and ExampleDocument8 pagesFMEA Form and Examplebenaoumeur benounaNo ratings yet
- American Trade Mark Order Form: Fill in Tag Color and Text BelowDocument1 pageAmerican Trade Mark Order Form: Fill in Tag Color and Text Belowbenaoumeur benounaNo ratings yet
- HIMT - MCA-AFF-HANDOUT - Page 1 - Created WithDocument1 pageHIMT - MCA-AFF-HANDOUT - Page 1 - Created Withbenaoumeur benounaNo ratings yet
- Fire Safety AwarenessDocument11 pagesFire Safety Awarenessbenaoumeur benounaNo ratings yet
- Cfo A Extinguisher ProtocolDocument135 pagesCfo A Extinguisher Protocolbenaoumeur benounaNo ratings yet
- PESTLE Analysis Template Version: DateDocument3 pagesPESTLE Analysis Template Version: Datebenaoumeur benounaNo ratings yet
- Semantic Feature Analysis TemplateDocument1 pageSemantic Feature Analysis Templatebenaoumeur benounaNo ratings yet
- Root Cause Analysis Investigation Report TemplateDocument3 pagesRoot Cause Analysis Investigation Report Templatebenaoumeur benounaNo ratings yet
- Break Even Analysis and MarkupDocument4 pagesBreak Even Analysis and Markupbenaoumeur benounaNo ratings yet
- Sub Module 1. PPEDocument20 pagesSub Module 1. PPEMutabazi Igga powersNo ratings yet
- Laporan Waktu Tunggu Operasi ElektifDocument22 pagesLaporan Waktu Tunggu Operasi Elektifeko saronoNo ratings yet
- 8 - InfanticideDocument7 pages8 - InfanticideAreej MohamedNo ratings yet
- Pinky - Plantar FasciitisDocument34 pagesPinky - Plantar FasciitisRavindra choudharyNo ratings yet
- Life 12 00188Document17 pagesLife 12 00188Ligia BoazuNo ratings yet
- New Disability Assessment Gazzette - 2024Document413 pagesNew Disability Assessment Gazzette - 2024nikkiNo ratings yet
- Chest TraumaDocument27 pagesChest TraumaGeraldine Marie SalvoNo ratings yet
- School Pothole LawsuitDocument6 pagesSchool Pothole LawsuitGreg DaileyNo ratings yet
- Decision Tree For Incident ClassificationDocument1 pageDecision Tree For Incident ClassificationAdrian BagayanNo ratings yet
- Uof Women'S Body Measuring Points DiagramDocument6 pagesUof Women'S Body Measuring Points DiagramLiyakath AliNo ratings yet
- Manual Operacion Dingli Manlift en E01-18Document93 pagesManual Operacion Dingli Manlift en E01-18Juan Pablo Monardez MaluendaNo ratings yet
- Assessment of Musculoskeletal Function Assessment of Musculoskeletal FunctionDocument22 pagesAssessment of Musculoskeletal Function Assessment of Musculoskeletal FunctionKaushena LindsayNo ratings yet
- Bruksanvisning 2377873 Pingi Vida2 Luftavfuktare 30 M 18 W SvartDocument40 pagesBruksanvisning 2377873 Pingi Vida2 Luftavfuktare 30 M 18 W SvartAleksandar LakicNo ratings yet
- Surface Anatomy of Upper LimbDocument19 pagesSurface Anatomy of Upper LimbAkomolede AbosedeNo ratings yet
- GALS ExamDocument6 pagesGALS ExamMaurensia MaurenNo ratings yet
- Bittner 2015 Acute and Perioperative Care of TheDocument34 pagesBittner 2015 Acute and Perioperative Care of TheJuan FelipeNo ratings yet
- Anatomy Physiology and Disease Foundations For The Health Professions 1St Edition Roiger Solutions Manual Full Chapter PDFDocument36 pagesAnatomy Physiology and Disease Foundations For The Health Professions 1St Edition Roiger Solutions Manual Full Chapter PDFcatherine.hanson719100% (16)
- Classification of Femur Trochanteric Fracture: Evaluating The Reliability of Tang ClassificationDocument6 pagesClassification of Femur Trochanteric Fracture: Evaluating The Reliability of Tang ClassificationMauricio ColoradoNo ratings yet
- IN THE COURT OF HON Respondent 1st CaseDocument12 pagesIN THE COURT OF HON Respondent 1st CaseAbhilash SaikiaNo ratings yet
- Hcai Pick ListDocument18 pagesHcai Pick ListKelly DanielssonNo ratings yet
- 0463 645 001 GBDocument38 pages0463 645 001 GBimreNo ratings yet