You might also like
- Assessment and Management of Peripheral Arterial Disease: What Every Cardiologist Should KnowDocument9 pagesAssessment and Management of Peripheral Arterial Disease: What Every Cardiologist Should KnowAlexandra NalgomNo ratings yet
- Guias ESC para Insuficiencia Cardiaca CronicaDocument128 pagesGuias ESC para Insuficiencia Cardiaca CronicaKarla HernandezNo ratings yet
- Medical Treatment of Aortic Stenosis: in DepthDocument19 pagesMedical Treatment of Aortic Stenosis: in DepthAlexandra NalgomNo ratings yet
- Abstract TG 68aDocument2 pagesAbstract TG 68aAlexandra NalgomNo ratings yet
- Henry FordDocument2 pagesHenry FordAlexandra NalgomNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- New Pe 2 Module DraftDocument29 pagesNew Pe 2 Module DraftSteffanie Michelle SabinoNo ratings yet
- MCQs on Chest Injuries and Thoracic SurgeryDocument35 pagesMCQs on Chest Injuries and Thoracic SurgeryFan Eli100% (15)
- Medical Transcription WorkbookDocument30 pagesMedical Transcription Workbookpbowen22333% (3)
- NMAT Part II Reviewer - PersonalDocument38 pagesNMAT Part II Reviewer - PersonalReycel MayNo ratings yet
- Anesthetic Aspects of The Fontan PatientDocument69 pagesAnesthetic Aspects of The Fontan PatientdavidmontoyaNo ratings yet
- Changes and signs of pregnancyDocument57 pagesChanges and signs of pregnancyth233No ratings yet
- - ملحق كونكت بلس excellenceDocument17 pages- ملحق كونكت بلس excellenceDinaNo ratings yet
- MODULE 2. (Legal Medicine)Document7 pagesMODULE 2. (Legal Medicine)Gina Cambongga100% (1)
- SCIENCE - LIGHT AND COLOURSDocument56 pagesSCIENCE - LIGHT AND COLOURSSoh Mei LingNo ratings yet
- R-Peak Time in Clinically Healthy Dogs With Different Thoracic ConformationsDocument5 pagesR-Peak Time in Clinically Healthy Dogs With Different Thoracic Conformationsayudantia uachNo ratings yet
- American Heart Association Guide to Auscultating the HeartDocument42 pagesAmerican Heart Association Guide to Auscultating the HeartHananya ManroeNo ratings yet
- Heart Sound .Mid Systolic Click-Mitral ProlapseDocument2 pagesHeart Sound .Mid Systolic Click-Mitral ProlapseTeti AndriNo ratings yet
- The Importance of A Healthy Respiratory SystemDocument10 pagesThe Importance of A Healthy Respiratory SystemRidhwan RosmanNo ratings yet
- Concept and Mapping For Rheumatic Heart DiseaseDocument5 pagesConcept and Mapping For Rheumatic Heart DiseaseAilyne A. CleofeNo ratings yet
- Checked - Unit 1 Molecules, Diet, Transport and Health - Exam - MSDocument16 pagesChecked - Unit 1 Molecules, Diet, Transport and Health - Exam - MSEllane leeNo ratings yet
- STUDENT-Eating - Disorder-F&E-UNFOLDING ReasoningDocument14 pagesSTUDENT-Eating - Disorder-F&E-UNFOLDING ReasoningPeggy100% (12)
- Circulatory System Multiple Choice QuestionsDocument4 pagesCirculatory System Multiple Choice QuestionsAlee MubeenNo ratings yet
- Signa HDXT 1.5T: See More, Do MoreDocument28 pagesSigna HDXT 1.5T: See More, Do MoreHoracio GomezNo ratings yet
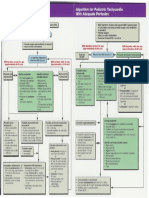
- Pediatric Tachycardia AlgorithmDocument1 pagePediatric Tachycardia AlgorithmGalih FatoniNo ratings yet
- Manual Twin Stim Plus Tens Ems Tif RusasDocument40 pagesManual Twin Stim Plus Tens Ems Tif RusasRodrigo Ivan Jara Puchi100% (2)
- Biology Paper 1Document32 pagesBiology Paper 1Cameron DaviesNo ratings yet
- A Case Study About Cardiovascular DiseaseDocument10 pagesA Case Study About Cardiovascular DiseaseBarben Balaquit100% (1)
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Echocardiography Assessment of Coronary Artery DiseaseDocument28 pagesEchocardiography Assessment of Coronary Artery DiseaseYibeltal AssefaNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Answer Key Nat ReviewerDocument19 pagesAnswer Key Nat ReviewerBASAY, HANNA RICA P.No ratings yet
- Cardiovascular System 101 Guided Notes 2Document3 pagesCardiovascular System 101 Guided Notes 2airihatsune21No ratings yet
- Possible Cardiac Chest Pain Clinical Pathway: FacilityDocument2 pagesPossible Cardiac Chest Pain Clinical Pathway: FacilityshofiyuddinNo ratings yet
- Pathology and Pathogenesis of Infective Endocarditis in Native Heart ValvesDocument8 pagesPathology and Pathogenesis of Infective Endocarditis in Native Heart ValvesIrina TănaseNo ratings yet
- Physiology PDFDocument34 pagesPhysiology PDFPipreNo ratings yet