You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BreastDocument8 pagesBreastNada MuchNo ratings yet
- Physiotherapy Patient History FormDocument5 pagesPhysiotherapy Patient History FormJean Pierre del Aguila MattaNo ratings yet
- Complete Pulse Diagnosis MethodsDocument7 pagesComplete Pulse Diagnosis MethodsSN WijesinheNo ratings yet
- MD Anderson Cancer Center Report On Trametes Versicolor Turkey Tail MushroomDocument14 pagesMD Anderson Cancer Center Report On Trametes Versicolor Turkey Tail MushroomMichaelNo ratings yet
- Arterial Blood Gas (ABG) AnalysisDocument18 pagesArterial Blood Gas (ABG) AnalysisAnandhu GNo ratings yet
- OET Writing Letter SampleDocument2 pagesOET Writing Letter Sampledrdk10% (1)
- BE HE@LTHY BE MOBILE A Handbook On How To Implement MCervicalCanceDocument47 pagesBE HE@LTHY BE MOBILE A Handbook On How To Implement MCervicalCancederr barrNo ratings yet
- Apac BFP 2015-16Document202 pagesApac BFP 2015-16derr barrNo ratings yet
- ANC Trends Uganda Oct11 2018Document36 pagesANC Trends Uganda Oct11 2018derr barrNo ratings yet
- Pathology-Based Research in AfricaDocument33 pagesPathology-Based Research in Africaderr barrNo ratings yet
- Key Facts: Adolescent PregnancyDocument10 pagesKey Facts: Adolescent Pregnancyderr barrNo ratings yet
- Accelerating Cervical Cancer Control and PreventionDocument2 pagesAccelerating Cervical Cancer Control and Preventionderr barrNo ratings yet
- The Message Box WorkbookDocument28 pagesThe Message Box Workbookderr barrNo ratings yet
- Message Box BlankDocument1 pageMessage Box Blankderr barrNo ratings yet
- 10 Tips To Winning A DELTAS Africa Grant - 0Document5 pages10 Tips To Winning A DELTAS Africa Grant - 0derr barrNo ratings yet
- DELTAS Africa II Budget Guidelines - Full ApplicationDocument2 pagesDELTAS Africa II Budget Guidelines - Full Applicationderr barrNo ratings yet
- Screening To Prevent Cancer DeathsDocument2 pagesScreening To Prevent Cancer Deathsderr barrNo ratings yet
- Adult Urology: ElsevierDocument6 pagesAdult Urology: Elsevierderr barrNo ratings yet
- Thomas McKeown A True Public Health PioneerDocument3 pagesThomas McKeown A True Public Health Pioneerderr barrNo ratings yet
- Cells Structure & FunctionDocument80 pagesCells Structure & Functionderr barrNo ratings yet
- Skin and Epithelial Tissues: Dr. Okello Michael / Dr. Mwaka ErisaDocument44 pagesSkin and Epithelial Tissues: Dr. Okello Michael / Dr. Mwaka Erisaderr barrNo ratings yet
- Protein Structurs and FunctionDocument54 pagesProtein Structurs and Functionderr barrNo ratings yet
- Dna Fingerprinting LabDocument37 pagesDna Fingerprinting Labderr barrNo ratings yet
- Metronidazole Vaginosis-1992Document4 pagesMetronidazole Vaginosis-1992maryNo ratings yet
- Euthanasia - Good DeathDocument16 pagesEuthanasia - Good DeathBernieNo ratings yet
- Prevention Management Obesity Children AdolescentsDocument20 pagesPrevention Management Obesity Children AdolescentsClaudia IrimieNo ratings yet
- Diagnosis and Management of Placenta PreviaDocument6 pagesDiagnosis and Management of Placenta PreviaNoveno Semestre FmuaqNo ratings yet
- Yimam Muhye 2018Document46 pagesYimam Muhye 2018Yayew MaruNo ratings yet
- Bahan Belajar Bersama SamaDocument55 pagesBahan Belajar Bersama SamakfcrajanyaayamNo ratings yet
- Menieres DiseaseDocument28 pagesMenieres DiseaseBonko Neville MengjoNo ratings yet
- Causes of Sterile Pyuria Infection RelatedDocument2 pagesCauses of Sterile Pyuria Infection RelatedSarah AhmedNo ratings yet
- Assessment (Cues) Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Interventions Rationale Evaluation SubjectiveDocument2 pagesAssessment (Cues) Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Interventions Rationale Evaluation SubjectiveJellaine Reyes AbarroNo ratings yet
- Hydro Treatments TariffsDocument2 pagesHydro Treatments TariffsLouvern MoodleyNo ratings yet
- Homoeopathy SummaryDocument9 pagesHomoeopathy SummaryFrancis LoboNo ratings yet
- Altered Mental State (Case Report)Document40 pagesAltered Mental State (Case Report)nugrahitaNo ratings yet
- Enfermedades de Transmision SexualDocument45 pagesEnfermedades de Transmision SexualGerardo LermaNo ratings yet
- PresbikusisDocument7 pagesPresbikusisLuluk AisyahNo ratings yet
- Seizure After StrokeDocument5 pagesSeizure After StrokeBrillyant S RaintamaNo ratings yet
- Pharmacology Chapter 3 and 4Document2 pagesPharmacology Chapter 3 and 4Dingal AijayNo ratings yet
- ARCADocument14 pagesARCADOMINGO CASANONo ratings yet
- What Causes IBS?Document4 pagesWhat Causes IBS?prima suci angrainiNo ratings yet
- Psychotherapeutic AgentsDocument2 pagesPsychotherapeutic AgentsjustinahorroNo ratings yet
- Tinospora Cordifolia - Uses and BenefitsDocument7 pagesTinospora Cordifolia - Uses and Benefitsjle_dlNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2021 OTOPHYNOPHARYNGOLOGYDocument6 pagesInformation MSQ KROK 2 Medicine 2007 2021 OTOPHYNOPHARYNGOLOGYReshma Shaji PnsNo ratings yet
- DPD and BPDDocument6 pagesDPD and BPDKamilah Haniyah MunawarNo ratings yet
- Pathophysiology of Alzheimers DiseaseDocument2 pagesPathophysiology of Alzheimers DiseaseJaysellePuguonTabijeNo ratings yet
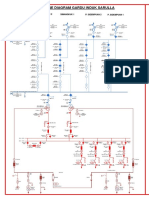
- SLD Gi SarullaDocument1 pageSLD Gi SarullasacilatwaeNo ratings yet