You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Cheese Making How-To'sDocument33 pagesCheese Making How-To'snikoskassNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pipe Network AnalysisDocument32 pagesPipe Network AnalysisRANJINI02VNo ratings yet
- Klangfarbenmelodie Amongst The Darmstadt Circle: Atmosphères at The Donaueschinger Musiktage, He WroteDocument48 pagesKlangfarbenmelodie Amongst The Darmstadt Circle: Atmosphères at The Donaueschinger Musiktage, He WroteBrandon McguireNo ratings yet
- 001 Art-AppreciationDocument13 pages001 Art-AppreciationBtrz QnnsNo ratings yet
- Handbook of Medical PhysicsDocument250 pagesHandbook of Medical PhysicsRana M ArslanNo ratings yet
- Unleash Your Speed: Thinking Forward. Challenging LimitsDocument3 pagesUnleash Your Speed: Thinking Forward. Challenging Limitsanon_19722876No ratings yet
- 106802-2727 Ijet-IjensDocument8 pages106802-2727 Ijet-IjensPrabakaran SubramaniamNo ratings yet
- Section 8. Loop TuningDocument22 pagesSection 8. Loop TuningakramhomriNo ratings yet
- Bahan PPT PPICDocument19 pagesBahan PPT PPICAoc SidomulyoNo ratings yet
- O RAN - WG3.E2SM RC R003 v04.00Document413 pagesO RAN - WG3.E2SM RC R003 v04.00animesh.vermaNo ratings yet
- Sap Faq FF ModuleDocument11 pagesSap Faq FF ModuleSharandeepNo ratings yet
- Edexcel IGCSE Unit 2E Homeostasis and Excretion - Self-Assessment SheetDocument6 pagesEdexcel IGCSE Unit 2E Homeostasis and Excretion - Self-Assessment SheetAli ALEBRAHIMNo ratings yet
- PROBABILITY It Is A Numerical Measure Which Indicates The ChanceDocument20 pagesPROBABILITY It Is A Numerical Measure Which Indicates The ChancePolice stationNo ratings yet
- Concepts in Balanced Device MeasurementsDocument12 pagesConcepts in Balanced Device MeasurementsA. VillaNo ratings yet
- Jee Main Sample Paper: Paper 1 For B.TechDocument22 pagesJee Main Sample Paper: Paper 1 For B.TechardhenduchatterjeeNo ratings yet
- Tutorials On MachinesDocument2 pagesTutorials On Machinesjenniferi_7No ratings yet
- Vocational Teacher (Maintenance and Repairs of Automobiles)Document7 pagesVocational Teacher (Maintenance and Repairs of Automobiles)Brandon AllenNo ratings yet
- AsasDocument180 pagesAsasAres SagaNo ratings yet
- Chapter 27 Analysis Edexcel Igcse Chemistry ReviewDocument14 pagesChapter 27 Analysis Edexcel Igcse Chemistry ReviewRafid Al NahiyanNo ratings yet
- MAPEH (Arts) : Quarter 2Document40 pagesMAPEH (Arts) : Quarter 2Eiay CommsNo ratings yet
- Renal Angiomyolipoma: Radiologic Classification and Imaging Features According To The Amount of FatDocument10 pagesRenal Angiomyolipoma: Radiologic Classification and Imaging Features According To The Amount of FatCarmen FandiñoNo ratings yet
- PWV3Document36 pagesPWV3Tony AppsNo ratings yet
- PA - 1d Progressing-workshop-V3Document12 pagesPA - 1d Progressing-workshop-V3hodubanjoNo ratings yet
- Vedic Maths 1Document5 pagesVedic Maths 1Ajmal AshrafNo ratings yet
- Chapter 11: Index NumberDocument7 pagesChapter 11: Index NumberHayati Aini AhmadNo ratings yet
- PCon - Planner System RequirementsDocument2 pagesPCon - Planner System RequirementsKristof MCNo ratings yet
- Mlion-Catalogue (2020)Document28 pagesMlion-Catalogue (2020)M.ariefiryuqoriNo ratings yet
- Prime NumbersDocument2 pagesPrime NumbersDarkas2100% (1)
- District Reading Monitoring and EvaluationDocument8 pagesDistrict Reading Monitoring and EvaluationMerafe Ebreo AluanNo ratings yet
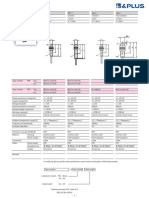
- B&Plus Proximity Sensor - 001.BES07e - Usm8-1Document1 pageB&Plus Proximity Sensor - 001.BES07e - Usm8-1Hussein RamzaNo ratings yet