You might also like
- Biomarkers, Diagnostics and Precision Medicine in the Drug Industry: Critical Challenges, Limitations and Roadmaps for the Best PracticesFrom EverandBiomarkers, Diagnostics and Precision Medicine in the Drug Industry: Critical Challenges, Limitations and Roadmaps for the Best PracticesNo ratings yet
- JNCI J Natl Cancer Inst 2009 Taube 1453 63Document11 pagesJNCI J Natl Cancer Inst 2009 Taube 1453 63Freddy A. ManayayNo ratings yet
- Integrating Biomarker Data in Clinical TrialsDocument5 pagesIntegrating Biomarker Data in Clinical TrialsSUMAN CHAUDHURINo ratings yet
- Advances in Biomarkers and Personalized MedicineDocument6 pagesAdvances in Biomarkers and Personalized MedicineEditor IJTSRDNo ratings yet
- Current PharmacoGenomics AssignmentDocument4 pagesCurrent PharmacoGenomics AssignmentShaher Bano MirzaNo ratings yet
- Bio Markers Its Novel ApplicationDocument7 pagesBio Markers Its Novel ApplicationPharmacognosy JournalNo ratings yet
- Drug Design and DevelopmentDocument5 pagesDrug Design and DevelopmentMark Russel Sean LealNo ratings yet
- Parkinson AccDocument13 pagesParkinson AccAlfiatur RizkiNo ratings yet
- Presented By: Anand Sagar Tiwari M.Pharm (Second Semester)Document56 pagesPresented By: Anand Sagar Tiwari M.Pharm (Second Semester)Dawit BirhanuNo ratings yet
- Importance of The Target Selection - Phase II FailuresDocument1 pageImportance of The Target Selection - Phase II FailuresSALEHA HASSANNo ratings yet
- Appi Ajp 2018 17111282Document14 pagesAppi Ajp 2018 17111282Alan AlvídrezNo ratings yet
- Pharmacogenetics Unlocking The Future of MedicineDocument7 pagesPharmacogenetics Unlocking The Future of MedicineErvin HoxhaNo ratings yet
- PharmacoDocument20 pagesPharmacoBrian OkariNo ratings yet
- Biomarkers in Clinical Medicine: Integration of Biomarkers Into Epidemiology Study DesignsDocument20 pagesBiomarkers in Clinical Medicine: Integration of Biomarkers Into Epidemiology Study DesignsGopika SureshNo ratings yet
- Genomic Biomarkers for Pharmaceutical Development: Advancing Personalized Health CareFrom EverandGenomic Biomarkers for Pharmaceutical Development: Advancing Personalized Health CareYihong YaoNo ratings yet
- PG14Document12 pagesPG14Nabila ChakourNo ratings yet
- Deep Learning in Pharmacogenomics: From Gene Regulation To Patient StratificationDocument40 pagesDeep Learning in Pharmacogenomics: From Gene Regulation To Patient StratificationSrikanth ShenoyNo ratings yet
- Personalized Medicines by Saumya DasDocument18 pagesPersonalized Medicines by Saumya DasSusmita GhoshNo ratings yet
- Post Marketing Surveillance and PharmacoepidemiologyDocument7 pagesPost Marketing Surveillance and PharmacoepidemiologyEditor IJTSRDNo ratings yet
- Methodology of Translational MedicineDocument83 pagesMethodology of Translational MedicineJosephChengNo ratings yet
- Biomarkers in Oncology Drug DevelopmentDocument9 pagesBiomarkers in Oncology Drug DevelopmentImola Al-KhzouzNo ratings yet
- Final BiomarkerDocument18 pagesFinal BiomarkerpareshtiwariNo ratings yet
- BMMDocument19 pagesBMMRitika agrawalNo ratings yet
- Note 1Document16 pagesNote 1nurul islamNo ratings yet
- Biomarkers – Unlocking Value in Early Drug DevelopmentDocument3 pagesBiomarkers – Unlocking Value in Early Drug DevelopmentSUMAN CHAUDHURINo ratings yet
- Report 2Document13 pagesReport 2api-3711225No ratings yet
- Early Drug Discovery ProcessDocument58 pagesEarly Drug Discovery ProcessFrietzyl Mae Generalao100% (1)
- Chapter 12 Systematic Review of Prognostic TestsDocument13 pagesChapter 12 Systematic Review of Prognostic TestsMuammar EmirNo ratings yet
- World Psychiatry - 2023 - Abi Dargham - Candidate Biomarkers in Psychiatric Disorders State of The FieldDocument27 pagesWorld Psychiatry - 2023 - Abi Dargham - Candidate Biomarkers in Psychiatric Disorders State of The FieldPranjal Sharma RNo ratings yet
- Biomarker-Based Drug Safety Assessment in The Age of Systems Pharmacology From Foundational To Regulatory ScienceDocument12 pagesBiomarker-Based Drug Safety Assessment in The Age of Systems Pharmacology From Foundational To Regulatory Scienceminglei.yeNo ratings yet
- PharmacoepidemiologyDocument2 pagesPharmacoepidemiologyFyrrNo ratings yet
- Cost and Effectiveness of Biologics For Rheumatoid Arthritis in A Commercially Insured PopulationDocument11 pagesCost and Effectiveness of Biologics For Rheumatoid Arthritis in A Commercially Insured PopulationAjeng DwiNo ratings yet
- Medication Safety: Improving Public HealthDocument6 pagesMedication Safety: Improving Public HealthViee Nie SfarmNo ratings yet
- Plants 11 03243Document28 pagesPlants 11 03243Rina HerowatiNo ratings yet
- Assessing The Value of Diagnostic Tests: A Framework For Designing and Evaluating TrialsDocument5 pagesAssessing The Value of Diagnostic Tests: A Framework For Designing and Evaluating TrialsMarisela FuentesNo ratings yet
- Studi Observasional Studi Eksperimental Syarat-Syarat Penelitian FarepidDocument12 pagesStudi Observasional Studi Eksperimental Syarat-Syarat Penelitian FarepidsanNo ratings yet
- Intro To Molecular DiagnosticsDocument39 pagesIntro To Molecular Diagnosticsmaxwell amponsahNo ratings yet
- Bio Marker 1Document11 pagesBio Marker 1Raluca Andreea AxinteNo ratings yet
- Fundamentalsof Pharmacogeneticsin Personalized, PrecisionmedicineDocument13 pagesFundamentalsof Pharmacogeneticsin Personalized, PrecisionmedicineSharanya ParamshettiNo ratings yet
- Precision Medicine For RheumatologistsDocument9 pagesPrecision Medicine For Rheumatologistsmihaelaatanasova123No ratings yet
- Role of Pharmacogenomics in Drug Discovery and Development: Review ArticleDocument7 pagesRole of Pharmacogenomics in Drug Discovery and Development: Review ArticleDrishti MohleyNo ratings yet
- Modeling & Simulation: ToolkitDocument24 pagesModeling & Simulation: ToolkitArchana MishraNo ratings yet
- Pharmacogenetics Clinical Decision Support SystemDocument32 pagesPharmacogenetics Clinical Decision Support Systemsavvy_as_98-1No ratings yet
- Approaches to setting health research prioritiesDocument13 pagesApproaches to setting health research prioritiesElla MaeNo ratings yet
- Pharmaco Epi Dam OlogyDocument40 pagesPharmaco Epi Dam OlogyJareena BegumNo ratings yet
- Health Technology Assessment To Assess Value of Biomarkers in The Decision-Making ProcessDocument8 pagesHealth Technology Assessment To Assess Value of Biomarkers in The Decision-Making Processgeo4maryNo ratings yet
- Pharmacogenomics DDI and DDGIDocument39 pagesPharmacogenomics DDI and DDGIMarfu'ah Mar'ahNo ratings yet
- Personalised Medicine Sem1Document19 pagesPersonalised Medicine Sem1RAKSHA ARUNNo ratings yet
- Pharmacogenetics Lecture NotesDocument5 pagesPharmacogenetics Lecture NotesMark Russel Sean LealNo ratings yet
- Overview of Drug Discovery and Development ProcessesDocument17 pagesOverview of Drug Discovery and Development ProcessesMelissa STanNo ratings yet
- Pharmaco GenomicsDocument14 pagesPharmaco GenomicsMarfu'ah Mar'ahNo ratings yet
- Drug Discovery Complete NotesDocument5 pagesDrug Discovery Complete NotesSadiqa ForensicNo ratings yet
- Biomarker Terminology Speaking The Same LanguageDocument12 pagesBiomarker Terminology Speaking The Same LanguageSuhendra Mandala ErnasNo ratings yet
- Chapter NO. Introduction To Pharmaceutical BiotechnologyDocument10 pagesChapter NO. Introduction To Pharmaceutical BiotechnologyM FaisalNo ratings yet
- CPT 1435 PDFDocument17 pagesCPT 1435 PDFarramithaNo ratings yet
- Pharmaco EpidemiologyDocument5 pagesPharmaco EpidemiologySUNIT ANANDNo ratings yet
- Sugammadex For Reversal of Rocuronium-Induced Neuromuscular Blockade in Pediatric PatientsDocument7 pagesSugammadex For Reversal of Rocuronium-Induced Neuromuscular Blockade in Pediatric PatientsAllonsiny GutierrezNo ratings yet
- The Impact of Health Information Technology On Patient SafetyDocument13 pagesThe Impact of Health Information Technology On Patient SafetySaba Abu FarhaNo ratings yet
- fvets-09-8604726Document10 pagesfvets-09-8604726drnguyenbvtkNo ratings yet
- Project Management Ebook FinalDocument22 pagesProject Management Ebook FinaldipanNo ratings yet
- Why Application Programming Interfaces Are Key For HealthcareDocument9 pagesWhy Application Programming Interfaces Are Key For HealthcareSUMAN CHAUDHURINo ratings yet
- The Most Common Issues in Submission DataDocument9 pagesThe Most Common Issues in Submission DataSUMAN CHAUDHURINo ratings yet
- What Does A Clinical Project Manager Do - Wake Forest University School of MedicineDocument5 pagesWhat Does A Clinical Project Manager Do - Wake Forest University School of MedicineSUMAN CHAUDHURINo ratings yet
- Why Choose Between SAS Data Step & PROC SQL When You Can Have BothDocument5 pagesWhy Choose Between SAS Data Step & PROC SQL When You Can Have BothSUMAN CHAUDHURINo ratings yet
- Implementation of ADaM Basic Data Structure On Genetic Variation Data For Pharmacogenomics StudiesDocument10 pagesImplementation of ADaM Basic Data Structure On Genetic Variation Data For Pharmacogenomics StudiesSUMAN CHAUDHURINo ratings yet
- Challenges and Strategies in PKPD ProgrammingDocument6 pagesChallenges and Strategies in PKPD ProgrammingSUMAN CHAUDHURINo ratings yet
- Implementation of STDM Pharmacogenomics - Genetics Domains On Genetic Variation DataDocument12 pagesImplementation of STDM Pharmacogenomics - Genetics Domains On Genetic Variation DataSUMAN CHAUDHURINo ratings yet
- The 5 Most Important Clinical SAS Programming Validation StepDocument6 pagesThe 5 Most Important Clinical SAS Programming Validation Steppalani.ramjiNo ratings yet
- Clinical Development Success Rates 2006-2015 - BIO, Biomedtracker, Amplion 2016 PDFDocument28 pagesClinical Development Success Rates 2006-2015 - BIO, Biomedtracker, Amplion 2016 PDFRibo SomaNo ratings yet
- Clinical Development Success Rates 2006-2015 - BIO, Biomedtracker, Amplion 2016 PDFDocument28 pagesClinical Development Success Rates 2006-2015 - BIO, Biomedtracker, Amplion 2016 PDFRibo SomaNo ratings yet
- REACTing To Data - The Use of Data Visualisation Within Early Clinical Statistical Programming at AZDocument6 pagesREACTing To Data - The Use of Data Visualisation Within Early Clinical Statistical Programming at AZSUMAN CHAUDHURINo ratings yet
- Biomarkers – Unlocking Value in Early Drug DevelopmentDocument3 pagesBiomarkers – Unlocking Value in Early Drug DevelopmentSUMAN CHAUDHURINo ratings yet
- Clinical Graphs Using SASDocument33 pagesClinical Graphs Using SASSUMAN CHAUDHURINo ratings yet
- Using CDISC Standards With An MDR For EDC To Submission TraceabilityDocument4 pagesUsing CDISC Standards With An MDR For EDC To Submission TraceabilitySUMAN CHAUDHURINo ratings yet
- Biomarker Qualification - Toward A Multiple Stakeholder Framework For Biomarker Development, Regulatory Acceptance, and UtilizationDocument13 pagesBiomarker Qualification - Toward A Multiple Stakeholder Framework For Biomarker Development, Regulatory Acceptance, and UtilizationSUMAN CHAUDHURINo ratings yet
- Clinical Database Metadata Quality Control With SAS® and PythonDocument16 pagesClinical Database Metadata Quality Control With SAS® and PythonSUMAN CHAUDHURINo ratings yet
- Real Time Clinical Trial Oversight With SASDocument7 pagesReal Time Clinical Trial Oversight With SASSUMAN CHAUDHURINo ratings yet
- PharmaSUG 2013 IB06Document10 pagesPharmaSUG 2013 IB06Palanivel GnanapragasamNo ratings yet
- Clinical Data Acquisition Standards Harmonization Importance and Benefits in Clinical Data ManagementDocument5 pagesClinical Data Acquisition Standards Harmonization Importance and Benefits in Clinical Data ManagementSUMAN CHAUDHURINo ratings yet
- Clinical Trial Data Integration - The Strategy, Benefits, and Logistics of Integrating Across A CompoundDocument12 pagesClinical Trial Data Integration - The Strategy, Benefits, and Logistics of Integrating Across A CompoundSUMAN CHAUDHURINo ratings yet
- Cdisc Standards - Explaining SDTM, Cdash, Adam, Odm-XML - AltexsoftDocument10 pagesCdisc Standards - Explaining SDTM, Cdash, Adam, Odm-XML - AltexsoftSUMAN CHAUDHURINo ratings yet
- Clinical Bioinformatics - A New Emerging ScienceDocument3 pagesClinical Bioinformatics - A New Emerging ScienceSUMAN CHAUDHURINo ratings yet
- Clinical Trial Reporting Using SASGRAPHDocument21 pagesClinical Trial Reporting Using SASGRAPHnathi_nathiNo ratings yet
- Clinical Database Metadata Quality Control With SAS® and PythonDocument16 pagesClinical Database Metadata Quality Control With SAS® and PythonSUMAN CHAUDHURINo ratings yet
- 195-2009 - Mapping CDISC Metadata Attributes - Using DATA - NULL - and PROC DATASETS in SAS®Document8 pages195-2009 - Mapping CDISC Metadata Attributes - Using DATA - NULL - and PROC DATASETS in SAS®SUMAN CHAUDHURINo ratings yet
- Clinical Trial Data Integration - The Strategy, Benefits, and Logistics of Integrating Across A CompoundDocument12 pagesClinical Trial Data Integration - The Strategy, Benefits, and Logistics of Integrating Across A CompoundSUMAN CHAUDHURINo ratings yet
- Introduction To SAS® Clinical Standards ToolkitDocument16 pagesIntroduction To SAS® Clinical Standards ToolkitSUMAN CHAUDHURINo ratings yet
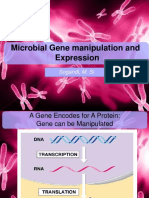
- Gene Manipulation and Expression TechniquesDocument40 pagesGene Manipulation and Expression TechniquesamandaNo ratings yet
- Anatomy and Physiology 1&2 (Part 1)Document117 pagesAnatomy and Physiology 1&2 (Part 1)Kleindyn Joy PeraltaNo ratings yet
- General Biology 1Document18 pagesGeneral Biology 1marushu valoNo ratings yet
- Isolate Bacterial Colonies Streak Plate MethodDocument5 pagesIsolate Bacterial Colonies Streak Plate MethodBryant Ken JavierNo ratings yet
- Blood Stain Analysis: HughesDocument8 pagesBlood Stain Analysis: HughesJesUs ChiQuez VenTuroNo ratings yet
- Grade 8 Science Olympiad WS2Document8 pagesGrade 8 Science Olympiad WS2Jithin RanganiNo ratings yet
- ADocument85 pagesAJake CopradeNo ratings yet
- Evolution and Consumer Behavior - Kristina M Durante and Vladas GriskeviciusDocument7 pagesEvolution and Consumer Behavior - Kristina M Durante and Vladas GriskeviciusR D PNo ratings yet
- Tehnologija Vode Za PiceDocument12 pagesTehnologija Vode Za PicejovanaNo ratings yet
- Microbilology - Unknown Lab ReportDocument2 pagesMicrobilology - Unknown Lab ReportAldenSchulteNo ratings yet
- The Embryology and Larval Development of The Goldfish (Carassius Auratus L.) From Lake ErieDocument13 pagesThe Embryology and Larval Development of The Goldfish (Carassius Auratus L.) From Lake EriealiefNo ratings yet
- Is Matter Around Us PureDocument188 pagesIs Matter Around Us Puresasi.curieNo ratings yet
- 36-PYSCH_Psychology-Key-Term-Glossary-Digital-Version_updatedDocument94 pages36-PYSCH_Psychology-Key-Term-Glossary-Digital-Version_updatedbasiaNo ratings yet
- Reading Exercises 0627Document22 pagesReading Exercises 0627lydianDNo ratings yet
- Role of Probiotics in AquacultureDocument24 pagesRole of Probiotics in AquacultureGopi NuthalapatiNo ratings yet
- Carlos Duarte Soundscape of The Anthropocene 2021Document12 pagesCarlos Duarte Soundscape of The Anthropocene 2021FedericoNo ratings yet
- Branches of Biology and Their MeaningDocument8 pagesBranches of Biology and Their MeaningSheena Llagas100% (1)
- Artigo OncoDocument14 pagesArtigo OncoCatarina LuísNo ratings yet
- 3rd Quarter Exam - Statistics and ProbabilityDocument11 pages3rd Quarter Exam - Statistics and ProbabilityLORENZO RAMIREZ100% (2)
- Regional Map Wide Bay Burnett Ed 8 Front 2009Document1 pageRegional Map Wide Bay Burnett Ed 8 Front 2009linNo ratings yet
- Cambridge International AS & A Level: Biology 9700/12Document20 pagesCambridge International AS & A Level: Biology 9700/12GiftElishaNdawalaNo ratings yet
- Laboratory Manual in Bio117.: Cell & Molecular Biology For Marine BiologyDocument6 pagesLaboratory Manual in Bio117.: Cell & Molecular Biology For Marine BiologyEnteña, Joana Jeanne L.No ratings yet
- Chapter Nine - Isolation, Culture and Propagation of Natural Killer CellsDocument11 pagesChapter Nine - Isolation, Culture and Propagation of Natural Killer CellsManoj Kumar pandreNo ratings yet
- Experimental Design GuideDocument21 pagesExperimental Design GuidemercyNo ratings yet
- Hegelian Theory Thesis Antithesis SynthesisDocument6 pagesHegelian Theory Thesis Antithesis Synthesismichelelataseattle100% (2)
- DISTRIBUSI SPASIAL IKAN BARONANG Siganus Canalicul PDFDocument18 pagesDISTRIBUSI SPASIAL IKAN BARONANG Siganus Canalicul PDFSantNo ratings yet
- Laboratory Manual and Workbook For Biological Anthropology 1st Edition Soluri Solutions ManualDocument25 pagesLaboratory Manual and Workbook For Biological Anthropology 1st Edition Soluri Solutions ManualAlexMartinxfgr100% (57)
- ZOOLOGYDocument123 pagesZOOLOGYWilver PascualNo ratings yet
- Suggestive Questions of Icse 2023 BiologyDocument5 pagesSuggestive Questions of Icse 2023 BiologySwethanaNo ratings yet
- Hydrocotyle vulgaris Essential Oil BioactivitiesDocument6 pagesHydrocotyle vulgaris Essential Oil BioactivitiesArmonNo ratings yet