You might also like
- RP Year 1 Semester 2Document234 pagesRP Year 1 Semester 2keith90% (10)
- Cooling Water Treatment PDFDocument2 pagesCooling Water Treatment PDFvjNo ratings yet
- Effect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleDocument6 pagesEffect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleRiefka Ananda ZulfaNo ratings yet
- Comment On “ The First 30  Years of TheDocument1 pageComment On “ The First 30  Years of TheYilianeth Mena DazaNo ratings yet
- Luminal BDocument6 pagesLuminal BPremiumstock90No ratings yet
- Ascha - ASJ19 - Nonsurgical Management of Facial Masculinization and FeminizationDocument15 pagesAscha - ASJ19 - Nonsurgical Management of Facial Masculinization and Feminizationallen.515No ratings yet
- Reaping The Benefits and Avoiding The Risks UnrealisticOptimism in The Health DomainDocument14 pagesReaping The Benefits and Avoiding The Risks UnrealisticOptimism in The Health DomainrayanNo ratings yet
- 11.the "Saw-It-All-Along" Effect Demonstrations of Visual Hindsight BiasDocument10 pages11.the "Saw-It-All-Along" Effect Demonstrations of Visual Hindsight BiasBlayel FelihtNo ratings yet
- JNMD DMM Cancer 2017Document6 pagesJNMD DMM Cancer 2017edtsendayushNo ratings yet
- Otolaryngol - Head Neck Surg - 2019 - Ellis - Body Image Disturbance in Surgically Treated Head and Neck Cancer Patients ADocument10 pagesOtolaryngol - Head Neck Surg - 2019 - Ellis - Body Image Disturbance in Surgically Treated Head and Neck Cancer Patients AJonas BorgesNo ratings yet
- ProposalDocument11 pagesProposalshoshoNo ratings yet
- Azad 2019Document7 pagesAzad 2019Eka BagaskaraNo ratings yet
- 10 1001@jamaoto 2015 0540 PDFDocument1 page10 1001@jamaoto 2015 0540 PDFAnonymous n1kgeSNo ratings yet
- Here Comes SummerDocument2 pagesHere Comes SummerLazar CrinaNo ratings yet
- Articles: BackgroundDocument15 pagesArticles: Backgroundvinadata01No ratings yet
- What Women Wish They Knew Before Prophylactic Mastectomy: B 2007 Wolters Kluwer Health - Lippincott Williams & WilkinsDocument7 pagesWhat Women Wish They Knew Before Prophylactic Mastectomy: B 2007 Wolters Kluwer Health - Lippincott Williams & WilkinsBusaina ANo ratings yet
- Clinical Optics: Basic and Clinical Science CourseDocument18 pagesClinical Optics: Basic and Clinical Science CourseIlham SamodraNo ratings yet
- Clinical Optics: Basic and Clinical Science CourseDocument18 pagesClinical Optics: Basic and Clinical Science CourseIlham SamodraNo ratings yet
- Introduction To Diagnostic RadiologyDocument702 pagesIntroduction To Diagnostic RadiologyPedro JoseNo ratings yet
- 12.patient Perspectives and Preferences For CommunicationDocument14 pages12.patient Perspectives and Preferences For Communicationbunga mawarNo ratings yet
- FDL 030Document6 pagesFDL 030panduranganNo ratings yet
- Venugopalan2016 PDFDocument7 pagesVenugopalan2016 PDFSyahidatul Kautsar NajibNo ratings yet
- A Model To Teach Elliptical Excision and Basic Suturing TechniquesDocument3 pagesA Model To Teach Elliptical Excision and Basic Suturing Techniques600WPMPONo ratings yet
- J Ijom 2020 06 020-2Document6 pagesJ Ijom 2020 06 020-2quajeutterugrau-6658No ratings yet
- Validación MASADocument10 pagesValidación MASAIgnacio AndresNo ratings yet
- Profess Use of Social MediaDocument7 pagesProfess Use of Social MediaGerardo ChavezNo ratings yet
- Expert Consensus Statement Management of Dysphagia in Head and Neck CancerDocument22 pagesExpert Consensus Statement Management of Dysphagia in Head and Neck CancerThomasMáximoMancinelliRinaldoNo ratings yet
- Screening Women at High Risk For Cervical CancerDocument6 pagesScreening Women at High Risk For Cervical CancerChristian Leonardo Molina HinojosaNo ratings yet
- Expert Recommendations On Use of Topical Therapeutics For Vitiligo in Pediatric, Adolescent, and Young Adult PatientsDocument9 pagesExpert Recommendations On Use of Topical Therapeutics For Vitiligo in Pediatric, Adolescent, and Young Adult Patientsjbahalkeh7570No ratings yet
- M CAD Ermatol: JA A DDocument4 pagesM CAD Ermatol: JA A DFa iNo ratings yet
- Guideline 2017 Autologous Breast ReconstructionDocument14 pagesGuideline 2017 Autologous Breast ReconstructionPedroAngelToribioOrbegozoNo ratings yet
- I2333 0406 21 4 LeeDocument7 pagesI2333 0406 21 4 LeePablo Segales BautistaNo ratings yet
- Screening For Psychosocial Distress A National SurDocument7 pagesScreening For Psychosocial Distress A National SurAlexNo ratings yet
- Maitake JSIODocument9 pagesMaitake JSIONICOLETANo ratings yet
- Effects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisDocument4 pagesEffects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisMiguel TuriniNo ratings yet
- Survey Analysis On The Management of Moderately DyDocument3 pagesSurvey Analysis On The Management of Moderately DyYilianeth Mena DazaNo ratings yet
- KAM Eng 2Document6 pagesKAM Eng 2Dóri PappNo ratings yet
- Factors Influencing Intention To Obtain The HPV Vaccine in South East Asian and Western Pacific Regions: A Systematic Review and Meta-AnalysisDocument11 pagesFactors Influencing Intention To Obtain The HPV Vaccine in South East Asian and Western Pacific Regions: A Systematic Review and Meta-AnalysispangaribuansantaNo ratings yet
- Christopher 2004Document12 pagesChristopher 2004katiane.souzaNo ratings yet
- Neral Medicine 8th EdDocument3,190 pagesNeral Medicine 8th EdValentina Galindo100% (3)
- Knowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsDocument7 pagesKnowledge of Chemotherapy and Occupational Safety Measures Among Nurses in Oncology UnitsIOM BNSNo ratings yet
- Guidelines of Care For The Management of Acne VulgarisDocument53 pagesGuidelines of Care For The Management of Acne VulgarisIuliana NitaNo ratings yet
- Harley Carlsen LoftusDocument9 pagesHarley Carlsen LoftusTri LacsonNo ratings yet
- 3.giacomami Users Quides To The MedicalDocument6 pages3.giacomami Users Quides To The MedicalMayra De LeonNo ratings yet
- ACR Criteria USDocument9 pagesACR Criteria USRenan LopesNo ratings yet
- Dribin 2020 - Persistent, Refractory, and Biphasic Anaphylaxis - A Multidisciplinary Delphi StudyDocument8 pagesDribin 2020 - Persistent, Refractory, and Biphasic Anaphylaxis - A Multidisciplinary Delphi StudygiadungdanamallNo ratings yet
- 2020 Book SkinDecontaminationDocument284 pages2020 Book SkinDecontaminationmespinozapiomboNo ratings yet
- NursingDocument9 pagesNursingpatel ravirajNo ratings yet
- An Evidence Based Scientific Analysis of Why Masks Are Ineffective Unnecessary and Harmful 10 12 2020 PDFDocument45 pagesAn Evidence Based Scientific Analysis of Why Masks Are Ineffective Unnecessary and Harmful 10 12 2020 PDFFiachMacNo ratings yet
- Jurnal Ca KulitDocument10 pagesJurnal Ca Kulitilham darnoNo ratings yet
- Ebn Presentation 1Document28 pagesEbn Presentation 1api-241721769No ratings yet
- 2016 EdBook PDFDocument931 pages2016 EdBook PDFambulatNo ratings yet
- Revista Paulista DE Pediatria: Triage and Risk Classification Protocols in Pediatric EmergencyDocument2 pagesRevista Paulista DE Pediatria: Triage and Risk Classification Protocols in Pediatric EmergencyAnonymous ONp8r5DkNo ratings yet
- Advances in Cosmetic Surgery Volume 2 2019 2019 Edition Edition Gregory H Branham Full ChapterDocument67 pagesAdvances in Cosmetic Surgery Volume 2 2019 2019 Edition Edition Gregory H Branham Full Chapteroscar.draper548100% (6)
- ASCCP Guidelines PDFDocument29 pagesASCCP Guidelines PDFmisstina.19876007No ratings yet
- Skin Cancer Prevention Education For Kidney Transplant Recipients: A Systematic Evaluation of Internet SitesDocument7 pagesSkin Cancer Prevention Education For Kidney Transplant Recipients: A Systematic Evaluation of Internet SitesPrathita AmandaNo ratings yet
- Safety in Radiation TherapyDocument2 pagesSafety in Radiation Therapyapi-571766863No ratings yet
- (Eason, 2021) 36Document3 pages(Eason, 2021) 36Corina Elena CozmaNo ratings yet
- Lipkus 2001Document8 pagesLipkus 2001irmNo ratings yet
- Nonsurgical Management of Facial Masculinization and Feminization PDFDocument15 pagesNonsurgical Management of Facial Masculinization and Feminization PDFImanuel CristiantoNo ratings yet
- RosaceaFrom EverandRosaceaJohn Havens CaryNo ratings yet
- Evidence-Based LaryngologyFrom EverandEvidence-Based LaryngologyDavid E. RosowNo ratings yet
- Impact of CoffeeDocument4 pagesImpact of CoffeeBryan NguyenNo ratings yet
- Ejhf 1858Document15 pagesEjhf 1858Bryan NguyenNo ratings yet
- Jacc: Heart Failure CmeDocument20 pagesJacc: Heart Failure CmeBryan NguyenNo ratings yet
- Unplanned Hospital Readmissions After Heartmate Ii ImplantationDocument9 pagesUnplanned Hospital Readmissions After Heartmate Ii ImplantationBryan NguyenNo ratings yet
- 1 s2.0 S221317791200008X MainDocument5 pages1 s2.0 S221317791200008X MainBryan NguyenNo ratings yet
- Aldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionDocument8 pagesAldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionBryan NguyenNo ratings yet
- Ciclosporin and Refractory Colitis.5Document6 pagesCiclosporin and Refractory Colitis.5Bryan NguyenNo ratings yet
- The Future of Cardiovascular BiomedicineDocument16 pagesThe Future of Cardiovascular BiomedicineBryan NguyenNo ratings yet
- A Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureDocument7 pagesA Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureBryan NguyenNo ratings yet
- Risk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyDocument12 pagesRisk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyBryan NguyenNo ratings yet
- Journal Pre-Proof: International Journal of Women's DermatologyDocument18 pagesJournal Pre-Proof: International Journal of Women's DermatologyBryan NguyenNo ratings yet
- Reasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsDocument9 pagesReasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsBryan NguyenNo ratings yet
- Clinical Implications of Abnormal Thyroid Function in Heart FailureDocument2 pagesClinical Implications of Abnormal Thyroid Function in Heart FailureBryan NguyenNo ratings yet
- Practice: Ulcerative Colitis: Diagnosis and ManagementDocument4 pagesPractice: Ulcerative Colitis: Diagnosis and ManagementBryan NguyenNo ratings yet
- MELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsDocument3 pagesMELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Original ResearchDocument4 pagesInternational Journal of Women's Dermatology: Original ResearchBryan NguyenNo ratings yet
- Update On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounDocument33 pagesUpdate On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounBryan NguyenNo ratings yet
- Feasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainDocument6 pagesFeasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainBryan NguyenNo ratings yet
- A Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsDocument9 pagesA Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Letters To The EditorDocument2 pagesInternational Journal of Women's Dermatology: Letters To The EditorBryan NguyenNo ratings yet
- Beasley-Meyer2010 Article CharacterizationOfTheUVAProtecDocument9 pagesBeasley-Meyer2010 Article CharacterizationOfTheUVAProtecBryan NguyenNo ratings yet
- 1 s2.0 S2352647521000538 MainDocument7 pages1 s2.0 S2352647521000538 MainBryan NguyenNo ratings yet
- The Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerDocument7 pagesThe Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerBryan NguyenNo ratings yet
- International Journal of Women's DermatologyDocument3 pagesInternational Journal of Women's DermatologyBryan NguyenNo ratings yet
- Clinical Profile of Melkersson-Rosenthal Syndrome/Orofacial Granulomatosis: A Review of 51 PatientsDocument7 pagesClinical Profile of Melkersson-Rosenthal Syndrome/Orofacial Granulomatosis: A Review of 51 PatientsBryan NguyenNo ratings yet
- PsoriDocument12 pagesPsoriBryan NguyenNo ratings yet
- Trends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosDocument6 pagesTrends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosBryan NguyenNo ratings yet
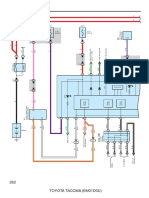
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- Group1 OB Ward-Case StudyDocument10 pagesGroup1 OB Ward-Case StudyAnthony Seth AguilandoNo ratings yet
- Drought Mandals of APDocument20 pagesDrought Mandals of APG Gopala Krishna GudladonaNo ratings yet
- BSBINews 78Document96 pagesBSBINews 78Anonymous dEztzVueNo ratings yet
- Lunch With AbbreviationsDocument2 pagesLunch With AbbreviationsthefallsteamNo ratings yet
- Simple Annuities FinalDocument95 pagesSimple Annuities FinalMae Ann KongNo ratings yet
- On Certain Modern Writers and The Institution of The Family - ChestertonDocument7 pagesOn Certain Modern Writers and The Institution of The Family - ChestertonMoldovan EdithNo ratings yet
- SanyyoGroup - Stone Crusher Plant 200 TPHDocument7 pagesSanyyoGroup - Stone Crusher Plant 200 TPHBagas Somporn Supriadi PutraNo ratings yet
- Classification of Tooth Preparations: Lecture Notes 2 DR - SuhadDocument6 pagesClassification of Tooth Preparations: Lecture Notes 2 DR - Suhadthomasw3No ratings yet
- Electrix TweakerDocument1 pageElectrix TweakerUSER58679No ratings yet
- Should We Encourage Research and Practice On Human CloningDocument3 pagesShould We Encourage Research and Practice On Human CloningMark Anthony Dela Cruz100% (1)
- UNIT 1-PHY 131 Chapter 2 - Introduction To VectorsDocument35 pagesUNIT 1-PHY 131 Chapter 2 - Introduction To VectorscharlieNo ratings yet
- Generator Breaker Equipped With Vacuum InterruptersDocument4 pagesGenerator Breaker Equipped With Vacuum InterruptersVenna Karthik ReddyNo ratings yet
- De KT Unit 1 - Tieng Anh 4 I-Learn Smart StartDocument6 pagesDe KT Unit 1 - Tieng Anh 4 I-Learn Smart Startmai anhNo ratings yet
- Seds QuizDocument5 pagesSeds QuizKaruNo ratings yet
- Introduction To Revit ArchitectureDocument99 pagesIntroduction To Revit ArchitectureOgunwusi Olubodun Samuel100% (1)
- Atex Directive in A NutshellDocument4 pagesAtex Directive in A NutshellAnonymous 96SYLheENo ratings yet
- Matrices Worksheet IDocument2 pagesMatrices Worksheet Icaroline_amideast8101No ratings yet
- Grade 5 Science Most Essential Learning Competencies MELCsDocument5 pagesGrade 5 Science Most Essential Learning Competencies MELCsPaul Fausto MaghirangNo ratings yet
- Fastback Slowback Soakback-CSURApr2014 RVHDocument14 pagesFastback Slowback Soakback-CSURApr2014 RVHJuan PabloNo ratings yet
- Yaksha Prashna Episode: MahabharataDocument18 pagesYaksha Prashna Episode: MahabharataSankar100% (1)
- Dirk The ProtectorDocument7 pagesDirk The ProtectorLyreNo ratings yet
- Biology I WorkbookDocument312 pagesBiology I Workbookchandra100% (3)
- An Alien HandDocument3 pagesAn Alien HandRini Sanjay PanikarNo ratings yet
- LanguageDocument8 pagesLanguageAlysson CamposNo ratings yet
- SurfaceDocument7 pagesSurfacestraihan234No ratings yet
- Genetic Calculator Help File: © 2016 K YorkeDocument18 pagesGenetic Calculator Help File: © 2016 K YorkeDan NegraiaNo ratings yet
- Instruction Manual AVTM246100B For Battery Ground Fault TracerDocument44 pagesInstruction Manual AVTM246100B For Battery Ground Fault TracerRovi ElecNo ratings yet