You might also like
- Ventricular Septal DefectDocument10 pagesVentricular Septal DefectSplenkerzRizkyWandaHikayaNo ratings yet
- Congenital Heart Disease GuideDocument89 pagesCongenital Heart Disease GuideMathew JosephNo ratings yet
- Microsoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFDocument51 pagesMicrosoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFHanafieHeluthNo ratings yet
- Atrial Septal DefectDocument13 pagesAtrial Septal DefectaudiNo ratings yet
- Radiology Write UpDocument28 pagesRadiology Write UpBong Peng DaNo ratings yet
- Ventricular Septal Defect-OverviewDocument42 pagesVentricular Septal Defect-OverviewRezwanul Hoque Bulbul100% (1)
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Cardiopatii Congenitale 17-18 enDocument74 pagesCardiopatii Congenitale 17-18 enMatei PopescuNo ratings yet
- jtd-10-S24-S2953Document13 pagesjtd-10-S24-S2953Faradiba MaricarNo ratings yet
- Cardiovascular Diseases VSD Asd 2022 1Document16 pagesCardiovascular Diseases VSD Asd 2022 1Boyu GrtrNo ratings yet
- Congenital Heart Disease - Part IDocument95 pagesCongenital Heart Disease - Part IMeraol HusseinNo ratings yet
- Ventricular Septal DefectDocument11 pagesVentricular Septal DefectFajar YuniftiadiNo ratings yet
- Congenital Heart Disease Acyanotic: Department of Cardiovascular Surgery St. George University General HospitalDocument81 pagesCongenital Heart Disease Acyanotic: Department of Cardiovascular Surgery St. George University General HospitalKonstantin DimitrovNo ratings yet
- Congenital Heart Disease GuideDocument77 pagesCongenital Heart Disease GuideMalueth Angui100% (1)
- Cctga PcicsDocument9 pagesCctga PcicsAdrian KhomanNo ratings yet
- Usm UvodDocument12 pagesUsm UvodMicija CucuNo ratings yet
- Ventricular Septal DefectDocument8 pagesVentricular Septal DefectWidelmark FarrelNo ratings yet
- Atrial Septal DefectDocument5 pagesAtrial Septal Defectalfiansyah syrfdnNo ratings yet
- Dr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshDocument48 pagesDr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshRezwanul Hoque Bulbul100% (1)
- IR 2022 Pediatric Nursing Handouts - Prof. Ma. Teresa VanguardiaDocument15 pagesIR 2022 Pediatric Nursing Handouts - Prof. Ma. Teresa VanguardiaJamie John EsplanadaNo ratings yet
- Acyanotic Congenital Heart DiseasesDocument255 pagesAcyanotic Congenital Heart DiseasesSarahNo ratings yet
- Resume AsdDocument32 pagesResume Asdanna prima sariNo ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- Aortopulmonary Window in InfantsDocument3 pagesAortopulmonary Window in Infantsonlyjust4meNo ratings yet
- Ongenital Eart Iseases: Iman Sulaiman Al-Hatmi 85569Document63 pagesOngenital Eart Iseases: Iman Sulaiman Al-Hatmi 85569Anişoara FrunzeNo ratings yet
- Pediatric ObjectivesDocument18 pagesPediatric Objectivesasheehan17No ratings yet
- Congenital Heart Disease Surgery TransDocument9 pagesCongenital Heart Disease Surgery TransPuguinGamingNo ratings yet
- Presented by Dona Mathew MSC (N) Govt - College of Nursing KottayamDocument221 pagesPresented by Dona Mathew MSC (N) Govt - College of Nursing KottayamSumathi GopinathNo ratings yet
- ASD Atrial Septal Defect PDFDocument9 pagesASD Atrial Septal Defect PDFAco AjjahNo ratings yet
- 22 Ventricular Septal DefectDocument26 pages22 Ventricular Septal Defectdhiraj parmarNo ratings yet
- Congenital Heart DiseaseDocument20 pagesCongenital Heart DiseaseMahdi AlattasNo ratings yet
- Congenital Heart Disease - Cynotic AcynoticDocument34 pagesCongenital Heart Disease - Cynotic Acynoticvruttika parmarNo ratings yet
- VSDDocument38 pagesVSDEva MegaNo ratings yet
- Question: Ostium Secondum Type of ASD: PrevalenceDocument9 pagesQuestion: Ostium Secondum Type of ASD: Prevalencesharon victoria mendezNo ratings yet
- Congenital Heart Disease GuideDocument66 pagesCongenital Heart Disease GuideMalueth AnguiNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- VSDDocument34 pagesVSDMerlina Wijayawati100% (2)
- Ventricular Septal Defects in AdultsDocument13 pagesVentricular Septal Defects in AdultsМихаил НеболеевNo ratings yet
- Research on causes and management of Atrial Septal Defect (ASDDocument3 pagesResearch on causes and management of Atrial Septal Defect (ASDJennifer FinnaliaNo ratings yet
- Congenital Heart Disease ExplainedDocument74 pagesCongenital Heart Disease ExplainedKeith LajotNo ratings yet
- Circulationaha 105 592055Document9 pagesCirculationaha 105 592055Simposium 214No ratings yet
- Pediatric Cardiology II Lecture SummaryDocument5 pagesPediatric Cardiology II Lecture SummaryMedisina101No ratings yet
- Lapkas Dian and DamboDocument34 pagesLapkas Dian and DamboDian Primadia PutriNo ratings yet
- Obstructive LesionsDocument7 pagesObstructive LesionsMaikka IlaganNo ratings yet
- DORVDocument5 pagesDORVkelly christyNo ratings yet
- Causes and Classification of Congenital Heart DefectsDocument27 pagesCauses and Classification of Congenital Heart DefectsNadiah Abdul HalimNo ratings yet
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Case Study: Double Outlet Right VentricleDocument6 pagesCase Study: Double Outlet Right VentriclejisooNo ratings yet
- Tetralogy of Fallot ExplainedDocument55 pagesTetralogy of Fallot ExplainedShravani ShagapuramNo ratings yet
- Congenital Heart DefectsDocument9 pagesCongenital Heart DefectsSHAMAE FAITH FARRENNo ratings yet
- PJB Pada Dewasa AASDocument54 pagesPJB Pada Dewasa AAS1e23e2ewNo ratings yet
- DR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentDocument58 pagesDR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentGomathi ShankarNo ratings yet
- VSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectDocument53 pagesVSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectAuni Akif AleesaNo ratings yet
- Eb SteinDocument112 pagesEb SteinAsena TuiketeiNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument7 pagesAcyanotic Congenital Heart DiseaseSam Raj100% (1)
- No L/R Ventricular HypertrophyDocument2 pagesNo L/R Ventricular HypertrophymcwnotesNo ratings yet
- Minggu 2 LP ASDDocument15 pagesMinggu 2 LP ASDMuhammad PanduNo ratings yet
- Anatomi dan Patofisiologi Aneurisma Sinus ValsalvaDocument16 pagesAnatomi dan Patofisiologi Aneurisma Sinus ValsalvaKhandar YosuaNo ratings yet
- Ventricular Septal DefectDocument18 pagesVentricular Septal DefectJessa Marie AgnesNo ratings yet
- PFO Risk Factor for StrokeDocument5 pagesPFO Risk Factor for StrokeAdrian KhomanNo ratings yet
- Pediatric Ocular Myastenia GravisDocument5 pagesPediatric Ocular Myastenia GravisAdrian KhomanNo ratings yet
- Pediatric Ocular Myastenia GravisDocument5 pagesPediatric Ocular Myastenia GravisAdrian KhomanNo ratings yet
- Pediatric Ocular Myastenia GravisDocument5 pagesPediatric Ocular Myastenia GravisAdrian KhomanNo ratings yet
- PFO Risk Factor for StrokeDocument5 pagesPFO Risk Factor for StrokeAdrian KhomanNo ratings yet
- Effectiveness of Simple Pediatric Rapid Response Team (PRRT) at COVID-19 Emergency Hospital Kemayoran (RSDCWAK)Document5 pagesEffectiveness of Simple Pediatric Rapid Response Team (PRRT) at COVID-19 Emergency Hospital Kemayoran (RSDCWAK)Adrian KhomanNo ratings yet
- Clinical Profiles of Pediatric Covid-19 at Covid-19 Emergency Hospital Kemayoran (RSDCWAK) : Following The Second Wave of Pandemic in IndonesiaDocument5 pagesClinical Profiles of Pediatric Covid-19 at Covid-19 Emergency Hospital Kemayoran (RSDCWAK) : Following The Second Wave of Pandemic in IndonesiaAdrian KhomanNo ratings yet
- Asterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriDocument5 pagesAsterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriAdrian KhomanNo ratings yet
- Primary Lymphoma of Bone in A 9 Years Old GirlDocument5 pagesPrimary Lymphoma of Bone in A 9 Years Old GirlAdrian KhomanNo ratings yet
- Meningococcal Infection in ChildrenDocument6 pagesMeningococcal Infection in ChildrenAdrian KhomanNo ratings yet
- Asterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriDocument5 pagesAsterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriAdrian KhomanNo ratings yet
- Clinical Profiles of Pediatric Covid-19 at Covid-19 Emergency Hospital Kemayoran (RSDCWAK) : Following The Second Wave of Pandemic in IndonesiaDocument5 pagesClinical Profiles of Pediatric Covid-19 at Covid-19 Emergency Hospital Kemayoran (RSDCWAK) : Following The Second Wave of Pandemic in IndonesiaAdrian KhomanNo ratings yet
- Effectiveness of Simple Pediatric Rapid Response Team (PRRT) at COVID-19 Emergency Hospital Kemayoran (RSDCWAK)Document5 pagesEffectiveness of Simple Pediatric Rapid Response Team (PRRT) at COVID-19 Emergency Hospital Kemayoran (RSDCWAK)Adrian KhomanNo ratings yet
- Primary Lymphoma of Bone in A 9 Years Old GirlDocument5 pagesPrimary Lymphoma of Bone in A 9 Years Old GirlAdrian KhomanNo ratings yet
- Raissa Virgy Rianda - Socio-Cultural and Economic Factors Impact To Children Malnutrition in Ksatria Airlangga Floating Hospital Service (RSTKA) in Remote Area - Bawean Island - Raissa RiandaDocument5 pagesRaissa Virgy Rianda - Socio-Cultural and Economic Factors Impact To Children Malnutrition in Ksatria Airlangga Floating Hospital Service (RSTKA) in Remote Area - Bawean Island - Raissa RiandaAdrian KhomanNo ratings yet
- PFO Risk Factor for StrokeDocument5 pagesPFO Risk Factor for StrokeAdrian KhomanNo ratings yet
- GAD65Ab Prevalence in Children with T1DMDocument5 pagesGAD65Ab Prevalence in Children with T1DMAdrian KhomanNo ratings yet
- Anthropometric Status Among Pediatric Patients with Transfusion-Dependent Beta-ThalassemiaDocument5 pagesAnthropometric Status Among Pediatric Patients with Transfusion-Dependent Beta-ThalassemiaAdrian KhomanNo ratings yet
- Konika Abstrak I Final (Edy Novery) - Compressed - Edy NoveryDocument5 pagesKonika Abstrak I Final (Edy Novery) - Compressed - Edy NoveryAdrian KhomanNo ratings yet
- Raissa Virgy Rianda - Socio-Cultural and Economic Factors Impact To Children Malnutrition in Ksatria Airlangga Floating Hospital Service (RSTKA) in Remote Area - Bawean Island - Raissa RiandaDocument5 pagesRaissa Virgy Rianda - Socio-Cultural and Economic Factors Impact To Children Malnutrition in Ksatria Airlangga Floating Hospital Service (RSTKA) in Remote Area - Bawean Island - Raissa RiandaAdrian KhomanNo ratings yet
- GAD65Ab Prevalence in Children with T1DMDocument5 pagesGAD65Ab Prevalence in Children with T1DMAdrian KhomanNo ratings yet
- Clinical Features and Outcomes of Childhood NP-SLEDocument5 pagesClinical Features and Outcomes of Childhood NP-SLEAdrian KhomanNo ratings yet
- Clinical Features and Outcomes of Childhood NP-SLEDocument5 pagesClinical Features and Outcomes of Childhood NP-SLEAdrian KhomanNo ratings yet
- Meningococcal Infection in ChildrenDocument6 pagesMeningococcal Infection in ChildrenAdrian KhomanNo ratings yet
- Pelod Vs Sofa Scoring in PediatricDocument6 pagesPelod Vs Sofa Scoring in PediatricAdrian KhomanNo ratings yet
- E-Poster Radiology AdhiniDocument5 pagesE-Poster Radiology AdhiniAdrian KhomanNo ratings yet
- Konika Abstrak I Final (Edy Novery) - Compressed - Edy NoveryDocument5 pagesKonika Abstrak I Final (Edy Novery) - Compressed - Edy NoveryAdrian KhomanNo ratings yet
- IVIG Administration Accelerate Recovery in Pediatric Miller Fisher Syndromes-A Case Report - Rahmad RamadhaniDocument5 pagesIVIG Administration Accelerate Recovery in Pediatric Miller Fisher Syndromes-A Case Report - Rahmad RamadhaniAdrian KhomanNo ratings yet
- Pediatric Pulmonary Hypertension - FullDocument67 pagesPediatric Pulmonary Hypertension - FullAlexandra Cortés ArciniegasNo ratings yet
- Case Report RetinoblastomaDocument5 pagesCase Report RetinoblastomaAdrian KhomanNo ratings yet
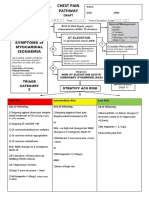
- Chest Pain Pathway GuideDocument4 pagesChest Pain Pathway GuidefauzanNo ratings yet
- Electrocardiogram: Dr. PacnaDocument13 pagesElectrocardiogram: Dr. PacnaEcel AggasidNo ratings yet
- Peripheral Vascular System Anatomy Exam TechniquesDocument2 pagesPeripheral Vascular System Anatomy Exam TechniquesAngelica Mae Dela CruzNo ratings yet
- 10.6 Health Issues Related To The Human Circulatory SystemDocument7 pages10.6 Health Issues Related To The Human Circulatory SystemrynNo ratings yet
- Acca Cs Syok SepsisDocument1 pageAcca Cs Syok SepsisSamuel KalonkNo ratings yet
- What Is Tetralogy of FallotDocument3 pagesWhat Is Tetralogy of FallotJyedenn PonceNo ratings yet
- Criterii de Acces Prioritar Stenoza MitralaDocument1 pageCriterii de Acces Prioritar Stenoza Mitralavasarhely imolaNo ratings yet
- Valvular Heart Disease Def PDFDocument3 pagesValvular Heart Disease Def PDFAfif Al BaalbakiNo ratings yet
- 1-7 Levick and Dwight - CardiovascularDocument7 pages1-7 Levick and Dwight - Cardiovascularrahmawati aliwarmanNo ratings yet
- Cardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityDocument35 pagesCardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityBarlonga Yhan YogaNo ratings yet
- Hemodynamic Unstable Patient Following ArrhythmiaDocument30 pagesHemodynamic Unstable Patient Following Arrhythmialew chin hongNo ratings yet
- Aortic DissectionDocument14 pagesAortic Dissectionapi-3733922100% (2)
- Case Report ASDDocument34 pagesCase Report ASDIrwansyah Ghenjy0% (1)
- Лекция 7Document76 pagesЛекция 7ramtin malekshahiNo ratings yet
- 1 - Pathophysiology of Cardiovascular SystemDocument63 pages1 - Pathophysiology of Cardiovascular SystemALNAKI0% (1)
- DR - Jetty - Executive Summary of Perioperative ManagementDocument28 pagesDR - Jetty - Executive Summary of Perioperative ManagementDilaNo ratings yet
- ACLS Practice Test2Document6 pagesACLS Practice Test2Ronald Rey Menor100% (11)
- Infective EndocarditisDocument3 pagesInfective EndocarditisAlfrin Antony80% (5)
- Cvs QuizDocument11 pagesCvs QuizSwamy KurnoolNo ratings yet
- LF01142&72 Ausc Smartsc 06 2019Document8 pagesLF01142&72 Ausc Smartsc 06 2019kkyenNo ratings yet
- PPTDocument8 pagesPPTArabelle TosocNo ratings yet
- CNS Pathology StrokeDocument11 pagesCNS Pathology StrokeKamran Khan KhalilNo ratings yet
- Examination CVS Case SheetDocument5 pagesExamination CVS Case Sheetsangeedh100% (2)
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 8Document9 pagesBetarie Anum Almira - RMIK (A) - Praktik KSPK 8Betarie Anum AlmiraNo ratings yet
- Approach To PalpitationsDocument2 pagesApproach To PalpitationsNicole Xyza JunsayNo ratings yet
- IsoketDocument2 pagesIsoketJaessa FelicianoNo ratings yet
- National CPR Association ACLS Study GuideDocument18 pagesNational CPR Association ACLS Study Guidekumar23No ratings yet
- Manage Hypertensive Crisis and Prevent Organ DamageDocument45 pagesManage Hypertensive Crisis and Prevent Organ DamageAndika HNo ratings yet
- Drugs Used in AnginaDocument24 pagesDrugs Used in AnginaChandra ShinodaNo ratings yet
- Nclex ExamDocument18 pagesNclex Examwaqas_xsNo ratings yet