You might also like
- Algorithm GERD Primary Care Pathway Ahs SCN DH 2020 15262Document7 pagesAlgorithm GERD Primary Care Pathway Ahs SCN DH 2020 15262Mihaela ShimanNo ratings yet
- GI Signs and SymptomsDocument40 pagesGI Signs and SymptomsJohnny BeeNo ratings yet
- Drugs in Psychiatric NursingDocument38 pagesDrugs in Psychiatric NursingJSeasharkNo ratings yet
- Irritable Bowel SyndromeDocument22 pagesIrritable Bowel SyndromeMarium NabeelNo ratings yet
- By Wisam Gatea HaniDocument32 pagesBy Wisam Gatea HanidrfatimarizNo ratings yet
- Irritable Bowel Syndrome-FINALDocument43 pagesIrritable Bowel Syndrome-FINALapi-3741769100% (2)
- Cocktail For Note 4Document52 pagesCocktail For Note 4Muhammad Bilal100% (3)
- Stool Examination - Part 1 - (Stool Analysis, Stool For Ova and Parasite, Stool Studies)Document11 pagesStool Examination - Part 1 - (Stool Analysis, Stool For Ova and Parasite, Stool Studies)Quennie Abellon QuimanNo ratings yet
- NCPDocument7 pagesNCPAbbie TantengcoNo ratings yet
- Rectal bleeding causes and treatment optionsDocument21 pagesRectal bleeding causes and treatment optionslinaleen67% (3)
- Dyspepsia ManagementDocument21 pagesDyspepsia Managementladyfame100% (1)
- Fungal Infections: Major Predisposing FactorsDocument6 pagesFungal Infections: Major Predisposing FactorsIsabel CastilloNo ratings yet
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)
- Diare Ubaya 2Document38 pagesDiare Ubaya 2indro hariantoNo ratings yet
- Diagnosis Dan Tatalaksana: Nyoman PurwadiDocument26 pagesDiagnosis Dan Tatalaksana: Nyoman PurwadiPande Indra PremanaNo ratings yet
- Duodenal UlcerDocument10 pagesDuodenal Ulcerfarha naazNo ratings yet
- IBS Presentation Week 213Document17 pagesIBS Presentation Week 213A MITCHELLNo ratings yet
- Irritable Bowel SyndromeDocument1 pageIrritable Bowel SyndromeYalin AbouhassiraNo ratings yet
- Ibdpresentation 140206191203 Phpapp01Document23 pagesIbdpresentation 140206191203 Phpapp01Christine MacGinnisNo ratings yet
- PGU VII 2019 The Role of Mabeverine in IBSDocument22 pagesPGU VII 2019 The Role of Mabeverine in IBSdiegoNo ratings yet
- PGU VII 2019 The Role of Mabeverine in IBSDocument22 pagesPGU VII 2019 The Role of Mabeverine in IBSdiegoNo ratings yet
- Abdominal pain - IBS checklistDocument3 pagesAbdominal pain - IBS checklistsalwakh266No ratings yet
- Lupus: Therapy T.Document10 pagesLupus: Therapy T.Sharifah ManuelNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Urosepsis With Aki On CKD: By-Roli JalanDocument79 pagesUrosepsis With Aki On CKD: By-Roli JalanRoli JalanNo ratings yet
- Otc Practice Lec 1Document54 pagesOtc Practice Lec 1mahgadNo ratings yet
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- Irritable Bowel SyndromeDocument8 pagesIrritable Bowel Syndrometaylor_holland_15No ratings yet
- Leshan Broniszewski-Burlingham Case Presentation 3 2017Document30 pagesLeshan Broniszewski-Burlingham Case Presentation 3 2017api-351417791No ratings yet
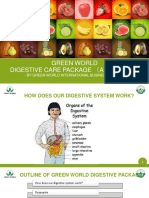
- Digestive Care Package AdvancedDocument22 pagesDigestive Care Package AdvancedWwNo ratings yet
- Irritable Bowel Syndrome: TitleDocument15 pagesIrritable Bowel Syndrome: TitleNorizam MorshidiNo ratings yet
- Adime 2Document13 pagesAdime 2api-496164982No ratings yet
- 2.6.3.7 Irritable Bowel Syndrom &kolitisDocument48 pages2.6.3.7 Irritable Bowel Syndrom &kolitisVaniNo ratings yet
- Crohns Disease FinalDocument3 pagesCrohns Disease Finalapi-535481376No ratings yet
- Case Study of UTIDocument6 pagesCase Study of UTIAmina TariqNo ratings yet
- Alcohol "Friend or Foe?'': Presented By: Isabel Athea VinasDocument56 pagesAlcohol "Friend or Foe?'': Presented By: Isabel Athea VinasIsabel VinasNo ratings yet
- What Is Irritable Bowel Syndrome and Who Gets It?: Do You Have IBS?Document6 pagesWhat Is Irritable Bowel Syndrome and Who Gets It?: Do You Have IBS?ThePhantomStrangerNo ratings yet
- Some Issues in The Management of Diarrhea in ChildrenDocument80 pagesSome Issues in The Management of Diarrhea in ChildrenRilie ArmeiliaNo ratings yet
- Im Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransDocument6 pagesIm Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransMelissa LabadorNo ratings yet
- Indian Female's Abdominal Pain and BreathlessnessDocument12 pagesIndian Female's Abdominal Pain and BreathlessnessayunisallehNo ratings yet
- Irritable Bowel SyndromeDocument12 pagesIrritable Bowel SyndromeSEIYADU IBRAHIM KNo ratings yet
- Dyspepsia LectureDocument2 pagesDyspepsia LectureDaneva Reyes0% (1)
- IBS: A Guide to Irritable Bowel SyndromeDocument38 pagesIBS: A Guide to Irritable Bowel SyndromeMuhammed sherbinNo ratings yet
- Doctor Charting Guidelines for HPI, Exams and ManagementDocument2 pagesDoctor Charting Guidelines for HPI, Exams and ManagementMacy Valenciano MacatuggalNo ratings yet
- PCT Pneumo ColonDocument16 pagesPCT Pneumo Colonsliding_doorsNo ratings yet
- Gastroenterology-Hepatology Division Internal Medicine Departement Fk-Usu/Adam Malik HospitalDocument30 pagesGastroenterology-Hepatology Division Internal Medicine Departement Fk-Usu/Adam Malik HospitalthelaziaNo ratings yet
- Physician's Orders for Admission and Treatment of Epigastric PainDocument4 pagesPhysician's Orders for Admission and Treatment of Epigastric PainJerremy LuqueNo ratings yet
- B.surrell IBSDocument53 pagesB.surrell IBSHeni PuspitasariNo ratings yet
- Drug OmeprazoleDocument1 pageDrug OmeprazoleSrkocherNo ratings yet
- Gastro DeliverableDocument4 pagesGastro DeliverableSandeep ShahNo ratings yet
- Case Srtudy of Hospital Work PDFDocument14 pagesCase Srtudy of Hospital Work PDFMagd NabilNo ratings yet
- Syndrome Neurotic 2Document5 pagesSyndrome Neurotic 2Msyr RaNo ratings yet
- Dyspepsia DiagnosticDocument71 pagesDyspepsia DiagnosticagilNo ratings yet
- Irritable Bowel SyndromeDocument11 pagesIrritable Bowel SyndromereboNo ratings yet
- International Journal of Nursing and Health Research: Management of Traveler's Diarrhea: Short ReviewDocument2 pagesInternational Journal of Nursing and Health Research: Management of Traveler's Diarrhea: Short ReviewAri PutraNo ratings yet
- Care Plan Template Long New PatDocument8 pagesCare Plan Template Long New Patchukwu.blessing4allNo ratings yet
- MEDICATIONSDocument3 pagesMEDICATIONSchristyNo ratings yet
- GastrolentrologyDocument38 pagesGastrolentrologyshaik.hossain2No ratings yet
- Irritable Bowel Syndrome: DiagnosisDocument11 pagesIrritable Bowel Syndrome: Diagnosisvenkatchem adiNo ratings yet
- Hyperemesis Gravidarum Case StudyDocument7 pagesHyperemesis Gravidarum Case StudyJose Carmelo JaramillaNo ratings yet
- Gerd - Peptic Ulcer - GastritisDocument87 pagesGerd - Peptic Ulcer - GastritisErickson V. LibutNo ratings yet
- Diagnosis and Management of Irritable Bowel Syndrome in Primary CareDocument2 pagesDiagnosis and Management of Irritable Bowel Syndrome in Primary CareBaghase PrasetyoNo ratings yet
- Drug OmeprazoleDocument1 pageDrug OmeprazoleSrkocherNo ratings yet
- Volvulus GROUP 4Document7 pagesVolvulus GROUP 41S VILLEGAS GabrielNo ratings yet
- A Dancing Patient: Dr. Ahmed Al MontasirDocument33 pagesA Dancing Patient: Dr. Ahmed Al MontasirMontasir AhmedNo ratings yet
- Pathway Gagal Ginjal Kronik: Intoleransi AktivitasDocument1 pagePathway Gagal Ginjal Kronik: Intoleransi AktivitasReza ApriandiNo ratings yet
- Chronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentDocument40 pagesChronic Venous Insufficiency: Causes, Symptoms, Diagnosis and TreatmentGihan NakhlehNo ratings yet
- Mucosta: Tablets 100mgDocument4 pagesMucosta: Tablets 100mgInukaicchi TakumichiNo ratings yet
- 7 MCQ UndergraduateDocument198 pages7 MCQ UndergraduateDrBasem89% (9)
- Pomfoliks JurnalDocument4 pagesPomfoliks JurnalTri RatnawatiNo ratings yet
- Integrated Therapeutics IiiDocument82 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Trematodes SummaryDocument6 pagesTrematodes SummaryabigailNo ratings yet
- Form Pg-Sga PDFDocument2 pagesForm Pg-Sga PDFzain syalsabila0% (1)
- Childhood Asthma: Symptoms, Causes, Risk Factors & ManagementDocument9 pagesChildhood Asthma: Symptoms, Causes, Risk Factors & ManagementJaved IqbalNo ratings yet
- DIURETICS Flow ChartDocument3 pagesDIURETICS Flow Chartdonnam86No ratings yet
- Epidemiology Related Terminology and Their DifferencesDocument3 pagesEpidemiology Related Terminology and Their DifferencesHasnat KhanNo ratings yet
- Ceftriaxone: An Update of Its Use in The Management of Community-Acquired and Nosocomial InfectionsDocument49 pagesCeftriaxone: An Update of Its Use in The Management of Community-Acquired and Nosocomial Infectionsjayswalramesh100% (2)
- MSDS Reach Potassium Silico FluorideDocument6 pagesMSDS Reach Potassium Silico Fluoridesamir5yNo ratings yet
- Obesidad Morbida.Document260 pagesObesidad Morbida.Mario LoyaNo ratings yet
- Toulmin Argument ModelDocument2 pagesToulmin Argument Modeljust_like_cake100% (1)
- GP Mental State Exam OSCEDocument2 pagesGP Mental State Exam OSCEJagdishVankar100% (1)
- Care For Critically Ill Patients With COVID-19: Clinical UpdateDocument2 pagesCare For Critically Ill Patients With COVID-19: Clinical UpdateNicole BatistaNo ratings yet
- 7 - Watterson and Kamradt-Scott - Fighting FluDocument24 pages7 - Watterson and Kamradt-Scott - Fighting FluSteffan Wyn-JonesNo ratings yet
- CCU CASE STUDY: STEMI POST CABGDocument26 pagesCCU CASE STUDY: STEMI POST CABGYousef JafarNo ratings yet
- The Creatine ReportDocument20 pagesThe Creatine ReportEnrique MerinoNo ratings yet
- Diseases of The Abomasum For Vet. Student by Ali SadiekDocument36 pagesDiseases of The Abomasum For Vet. Student by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Inflammatory Bowel DiseaseDocument412 pagesInflammatory Bowel DiseaseSabbra CadabraNo ratings yet
- Neet Pedigree Questions Worksheet 5ef6eb6eca031Document8 pagesNeet Pedigree Questions Worksheet 5ef6eb6eca031sarudarshinij.s123No ratings yet
- MeniereDocument5 pagesMeniereMayls Sevilla CalizoNo ratings yet