You might also like
- Post-Traumatic Stress Disorder Workbook: Practical Help and Information for PTSDFrom EverandPost-Traumatic Stress Disorder Workbook: Practical Help and Information for PTSDRating: 4.5 out of 5 stars4.5/5 (6)
- The Health Effects of Cannabis and Cannabinoids (2017)Document395 pagesThe Health Effects of Cannabis and Cannabinoids (2017)Cannabis Israel100% (3)
- AnxietyDocument40 pagesAnxietyhelperforeu100% (2)
- The Safe Guide: To Heal Trauma & AttachmentDocument25 pagesThe Safe Guide: To Heal Trauma & AttachmentSunay100% (4)
- COVID19 Critical Illness Intensive Care PTSDDocument31 pagesCOVID19 Critical Illness Intensive Care PTSDCherylNo ratings yet
- Post Traumatic Stress: An NHS Self Help GuideDocument28 pagesPost Traumatic Stress: An NHS Self Help GuideKristine Apostol RecanaNo ratings yet
- Anxiety and Panic Attacks 2021 PDF VersionDocument23 pagesAnxiety and Panic Attacks 2021 PDF VersionArwind RoyNo ratings yet
- Anxiety and Panic AttacksDocument21 pagesAnxiety and Panic AttacksAngelica NicholeNo ratings yet
- Trauma and Coping StrategiesDocument12 pagesTrauma and Coping StrategiesProf. Lakshman Madurasinghe100% (23)
- What? Me Worry!?! What? Me Worry!?!Document7 pagesWhat? Me Worry!?! What? Me Worry!?!KonkmanNo ratings yet
- Anxiety DisorderDocument36 pagesAnxiety DisorderRujuta BaramateNo ratings yet
- The Suicide Assessment ScaleDocument15 pagesThe Suicide Assessment ScaleOti VuraNo ratings yet
- Anxiety 1Document7 pagesAnxiety 1Mustafa HusseinNo ratings yet
- PPP Training Module 3 FINAL - JanDocument41 pagesPPP Training Module 3 FINAL - JanMary Ann MejiaNo ratings yet
- Unraveling The Tangles of AnxietyDocument24 pagesUnraveling The Tangles of AnxietyIbiba GeorgeNo ratings yet
- 01 Overview of General Is Ed AnxietyDocument7 pages01 Overview of General Is Ed AnxietyMirjam LipstokNo ratings yet
- Gad 1 2015 Gad PDFDocument7 pagesGad 1 2015 Gad PDFLindseyRae ParkerNo ratings yet
- What Me Worry - 01 - Overview of Generalised AnxietyDocument7 pagesWhat Me Worry - 01 - Overview of Generalised AnxietyManda BlaževićNo ratings yet
- Psychological Responses To Traumatic Stress: What To ExpectDocument3 pagesPsychological Responses To Traumatic Stress: What To Expectcitalac69No ratings yet
- Anxiety Disorders and Anxiety AttacksDocument11 pagesAnxiety Disorders and Anxiety AttacksBrgy BalolingNo ratings yet
- Anxiety Sue HughesDocument20 pagesAnxiety Sue HughesAna-Maria DeciuNo ratings yet
- What Me Worry - 01 - Overview of Generalised Anxiety-2Document7 pagesWhat Me Worry - 01 - Overview of Generalised Anxiety-2장채윤No ratings yet
- Anxiety Disorders: Emotional Symptoms of AnxietyDocument7 pagesAnxiety Disorders: Emotional Symptoms of AnxietyRussel TalastasNo ratings yet
- PPP Training Module 3 DownloadDocument46 pagesPPP Training Module 3 DownloadNafiu AbdullateefNo ratings yet
- Student Self-Care ManualDocument79 pagesStudent Self-Care Manualpriskilahilary100% (3)
- Ryle S. Jacinto: 12-HumanityDocument6 pagesRyle S. Jacinto: 12-HumanityPauloXander LozanoNo ratings yet
- An Anxiety Journal: 10 Signs To Discover Your Anxiety And How Bad It Can Hurt YouFrom EverandAn Anxiety Journal: 10 Signs To Discover Your Anxiety And How Bad It Can Hurt YouNo ratings yet
- Workbook For The Body Keeps The ScoreDocument111 pagesWorkbook For The Body Keeps The ScoreMyrto Papadaki100% (2)
- HERO-Ethiopia Module 2Document24 pagesHERO-Ethiopia Module 2RahelAdmasuNo ratings yet
- Post Traumatic Stress Disorder: Merin Solomon MSC Nursing Vijaya College of NursingDocument28 pagesPost Traumatic Stress Disorder: Merin Solomon MSC Nursing Vijaya College of Nursingmerin sunilNo ratings yet
- Infosheet On Anxiety - 2Document4 pagesInfosheet On Anxiety - 2Ale ValdésNo ratings yet
- What Are Anxiety Disorders/depressions?Document2 pagesWhat Are Anxiety Disorders/depressions?Cams BlogNo ratings yet
- Coping With PTSD Trauma1704206530Document4 pagesCoping With PTSD Trauma1704206530phani BhushanNo ratings yet
- Mindfulness: Mindfulness For Anxiety Relief How To Use Mindfulness Based Stress Reduction Meditation Exercises To Develop Peace and Happiness In Your Everyday LifeFrom EverandMindfulness: Mindfulness For Anxiety Relief How To Use Mindfulness Based Stress Reduction Meditation Exercises To Develop Peace and Happiness In Your Everyday LifeNo ratings yet
- Converging The Mind & Body for Healing: Self-healing, Healing Trauma, Reducing Suffering & Reclaiming your LifeFrom EverandConverging The Mind & Body for Healing: Self-healing, Healing Trauma, Reducing Suffering & Reclaiming your LifeNo ratings yet
- Anxiety PDFDocument2 pagesAnxiety PDFHussain OtlaNo ratings yet
- Anxiety PDFDocument2 pagesAnxiety PDFHussain OtlaNo ratings yet
- Antenatal Anxiety Consumer Fact SheetDocument3 pagesAntenatal Anxiety Consumer Fact SheetjosawoodNo ratings yet
- PTSD 4pageDocument4 pagesPTSD 4pageKrause KarlNo ratings yet
- HERO-Ethiopia Module 3Document31 pagesHERO-Ethiopia Module 3RahelAdmasuNo ratings yet
- Anxiety Disorders Are A Group ofDocument3 pagesAnxiety Disorders Are A Group ofLime MNo ratings yet
- Overcome Anxiety: How to Stop The Cycle of Anxiety, Worry and Fear So You Can Regain Control of Your LifeFrom EverandOvercome Anxiety: How to Stop The Cycle of Anxiety, Worry and Fear So You Can Regain Control of Your LifeNo ratings yet
- Anxiety Disorder Performance Task 1Document15 pagesAnxiety Disorder Performance Task 1hadukenNo ratings yet
- Lesson - 07 CBTDocument30 pagesLesson - 07 CBTRitesh WaghmareNo ratings yet
- Conversion Disorder Hysterical NeurosisDocument4 pagesConversion Disorder Hysterical NeurosisrianachuNo ratings yet
- Anxiety Disorders FactsheetDocument22 pagesAnxiety Disorders FactsheetHigazi z'EagleNo ratings yet
- Stop the Fear: Learn to Stop Anxiety Panic Attacks and Take Control of Your LifeFrom EverandStop the Fear: Learn to Stop Anxiety Panic Attacks and Take Control of Your LifeNo ratings yet
- Understanding Post-Traumatic Stress: A Normal Reaction To Abnormal EventsDocument6 pagesUnderstanding Post-Traumatic Stress: A Normal Reaction To Abnormal EventsGabita31No ratings yet
- Headlines Guide To Vicarious TraumaDocument20 pagesHeadlines Guide To Vicarious TraumaElvis Posada QuirogaNo ratings yet
- The Positive Side To Your AnxietyDocument4 pagesThe Positive Side To Your AnxietyKathy Campos RaymundoNo ratings yet
- 2nd Week PresentationDocument30 pages2nd Week PresentationRevina LabradorNo ratings yet
- AnxietyDocument16 pagesAnxietyNiharikaNo ratings yet
- MR21npE3Eem xg4p7cmXwA - Module 9 Lecture 1Document16 pagesMR21npE3Eem xg4p7cmXwA - Module 9 Lecture 1Edward RamirezNo ratings yet
- Generalized Anxiety Disorder - Patient Treatment ManualDocument72 pagesGeneralized Anxiety Disorder - Patient Treatment ManualPriya Puri100% (1)
- The Anxiety and Panic Attacks Toolbox of Cures: The anti-anxiety healers guide book & first aid kit for extreme anxiety relief, cbt, diet, plus a survival guide toolkit for teens, adults & kidsFrom EverandThe Anxiety and Panic Attacks Toolbox of Cures: The anti-anxiety healers guide book & first aid kit for extreme anxiety relief, cbt, diet, plus a survival guide toolkit for teens, adults & kidsNo ratings yet
- 01 Session 05 Anxiety and FearDocument62 pages01 Session 05 Anxiety and FearMalakatete Mwaipojele-fNo ratings yet
- Im So Stressed OutDocument2 pagesIm So Stressed OutAlexandra whimsicalNo ratings yet
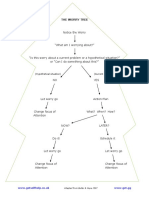
- Worry TreeDocument1 pageWorry TreeSunayNo ratings yet
- Users Guide & Installation Handbook: Stoves Freestanding Dual Fuel Wok UKDocument44 pagesUsers Guide & Installation Handbook: Stoves Freestanding Dual Fuel Wok UKSunayNo ratings yet
- Guideline: Breastfeeding in FacilitiesDocument136 pagesGuideline: Breastfeeding in FacilitiesServoplant SrlNo ratings yet
- Daily Iron Supplementation PDFDocument54 pagesDaily Iron Supplementation PDFadhiNo ratings yet
- In Our Food: PesticidesDocument2 pagesIn Our Food: PesticidesSunayNo ratings yet
- Timothy Snyder, 20 Lessons From The 20thINGLÊS PDFDocument48 pagesTimothy Snyder, 20 Lessons From The 20thINGLÊS PDFGabriel OliveiraNo ratings yet
- Assange Nasrallah Broadcast InterviewDocument6 pagesAssange Nasrallah Broadcast InterviewjohnnystulicNo ratings yet
- (Intravenous Fluids) : Cellular Fluid CompartmentsDocument17 pages(Intravenous Fluids) : Cellular Fluid CompartmentsFatimaNo ratings yet
- Lab 7 NewDocument3 pagesLab 7 New202010187No ratings yet
- Childhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenDocument9 pagesChildhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenScott PymNo ratings yet
- Kegawatdaruratan Asma Dan PPOKDocument27 pagesKegawatdaruratan Asma Dan PPOKPark JiminNo ratings yet
- Unit 10-Maintain Knowledge of Improvements To Influence Health and Safety Practice RGDocument10 pagesUnit 10-Maintain Knowledge of Improvements To Influence Health and Safety Practice RGAshraf EL WardajiNo ratings yet
- Fdar Psychiatric DutyDocument2 pagesFdar Psychiatric DutyErica Maceo MartinezNo ratings yet
- Anxiety Scales Used in Pregnancy Systematic ReviewDocument13 pagesAnxiety Scales Used in Pregnancy Systematic ReviewFera NovalinaNo ratings yet
- Barangay Council For The Protection of ChildrenDocument6 pagesBarangay Council For The Protection of ChildrenGem BesandeNo ratings yet
- Director Hertel LetterDocument2 pagesDirector Hertel LetterWWMTNo ratings yet
- Template Traffic Light MatrixDocument1 pageTemplate Traffic Light MatrixDivalita100% (1)
- Ocde TurismoDocument19 pagesOcde TurismoPedro MentadoNo ratings yet
- Reopening Church After CovidDocument26 pagesReopening Church After CovidhmareidNo ratings yet
- The Maudsley Model of FTDocument8 pagesThe Maudsley Model of FTCandela SánchezNo ratings yet
- Toolbox Talks - Near Miss ReportingDocument1 pageToolbox Talks - Near Miss ReportinganaNo ratings yet
- Rosenbaum M Capstone Clinical Case StudyDocument16 pagesRosenbaum M Capstone Clinical Case Studyapi-531827736No ratings yet
- Zoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Document2 pagesZoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Eileen Le RouxNo ratings yet
- Pharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Document11 pagesPharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Md. Akil Mahmud100% (1)
- Respiratory DistressDocument34 pagesRespiratory DistressSindhiya DurairajanNo ratings yet
- Https Icar - Nta.ac - in Icarugadmitcard2021 Printout - Aspx Skey 637662179022622761Document4 pagesHttps Icar - Nta.ac - in Icarugadmitcard2021 Printout - Aspx Skey 637662179022622761Zoya AkhtarNo ratings yet
- RADIOLOGY 1.6 Introduction To MammographyDocument9 pagesRADIOLOGY 1.6 Introduction To MammographyZazaNo ratings yet
- Chulabhorn Graduate Institute Post-Graduate Scholarship Program Scholarship Application Form (For NON-ASEAN Applicants)Document5 pagesChulabhorn Graduate Institute Post-Graduate Scholarship Program Scholarship Application Form (For NON-ASEAN Applicants)maha AbdulazizNo ratings yet
- Detail of Rajiv Gandhi Jeevandayee Arogya Yojana MaharashtraDocument180 pagesDetail of Rajiv Gandhi Jeevandayee Arogya Yojana MaharashtraBrandon Bell100% (1)
- Defecography: Technique, Interpretation, and Current Use: Arden M. Morris and Susan C. ParkerDocument14 pagesDefecography: Technique, Interpretation, and Current Use: Arden M. Morris and Susan C. ParkerSuraj KurmiNo ratings yet
- Msds - Pasta Tomate. (Ingles)Document4 pagesMsds - Pasta Tomate. (Ingles)Yanina GutierrezNo ratings yet
- Module 3 FP Client AssessmentDocument54 pagesModule 3 FP Client AssessmentJhunna TalanganNo ratings yet
- Achilles Tendon Forces and Pain During Common RehabilitationDocument8 pagesAchilles Tendon Forces and Pain During Common RehabilitationIan JuanicoNo ratings yet
- Abnormal Psychology: Prof: Shwetha MuraliDocument55 pagesAbnormal Psychology: Prof: Shwetha MuraliANCHITA THIAGARAJANNo ratings yet
- OA1 Grammar Worksheets FinalDocument17 pagesOA1 Grammar Worksheets FinalGabriela Paola CUELLONo ratings yet
- Penguard Tie Coat 100: Technical Data Sheet Application GuideDocument7 pagesPenguard Tie Coat 100: Technical Data Sheet Application GuideIrawan FajarNo ratings yet
- PHED To PATHFITDocument4 pagesPHED To PATHFITGraceNo ratings yet