You might also like
- Lecture 7 Acupuncture Acupressure 2020S2 - StudentDocument39 pagesLecture 7 Acupuncture Acupressure 2020S2 - StudentAyeitzreg100% (2)
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Chronic PancreatitisDocument42 pagesChronic PancreatitismmurugeshrajNo ratings yet
- A Concept Map On External OtitisDocument9 pagesA Concept Map On External OtitisJoe RealNo ratings yet
- Hearing LossDocument31 pagesHearing LossDat boi100% (1)
- 2016 OITE Study Guide For ResidentsDocument273 pages2016 OITE Study Guide For Residentschu_chiang_3100% (1)
- Health Law BibliographyDocument11 pagesHealth Law BibliographyIeien MuthmainnahNo ratings yet
- Diseases of Periradicular TissuesDocument62 pagesDiseases of Periradicular Tissuesanubhutigupta1404No ratings yet
- Vestibular Neutitis & Labyrinthitis PDFDocument6 pagesVestibular Neutitis & Labyrinthitis PDFFika Khulma SofiaNo ratings yet
- Otosclerosis and Menieres DiseaseDocument5 pagesOtosclerosis and Menieres DiseaseYoko Mae YanoNo ratings yet
- International Days CalendarDocument6 pagesInternational Days CalendarCorkChoral0% (1)
- Strovac Prospect EnglishDocument6 pagesStrovac Prospect EnglishSorin Rusu75% (4)
- Pemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanDocument71 pagesPemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanRilianda SimbolonNo ratings yet
- Bulvar and Psevdobulbar SyndromeDocument4 pagesBulvar and Psevdobulbar SyndromeresearchparksNo ratings yet
- Hearing Loss (Badhirya) and Its Ayurvedic Management: A Case StudyDocument9 pagesHearing Loss (Badhirya) and Its Ayurvedic Management: A Case Studyshweta kotwal100% (1)
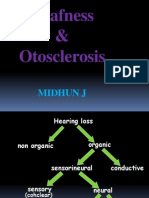
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- Inflammatory Infection and Trauma of The Middle EarDocument27 pagesInflammatory Infection and Trauma of The Middle EarChristelle Ann FarralesNo ratings yet
- Un Cas Exceptionnel D'aréflexie Vestibulaire Bilatérale Compliquant Une Otite Moyenne AiguëDocument4 pagesUn Cas Exceptionnel D'aréflexie Vestibulaire Bilatérale Compliquant Une Otite Moyenne AiguëHabib CHEIKH EL WELYNo ratings yet
- Skull Base Osteomyelitis: A Comprehensive Imaging Review: SummaryDocument10 pagesSkull Base Osteomyelitis: A Comprehensive Imaging Review: SummaryDupilumab DupilumabNo ratings yet
- Disability AssignmentDocument15 pagesDisability AssignmentJusy BinguraNo ratings yet
- Microtia-The Most Frequent Congenital Abnormality of The External Ear and Its Clinical SignificanceDocument9 pagesMicrotia-The Most Frequent Congenital Abnormality of The External Ear and Its Clinical SignificanceMuhammad Syamirul AlamNo ratings yet
- 135 Infections of The External EarDocument12 pages135 Infections of The External EarDickyJuliandaNo ratings yet
- Otitis EksternaDocument6 pagesOtitis EksternaranmiNo ratings yet
- Hearing Loss SMT IV44Document94 pagesHearing Loss SMT IV44abdul fattah mufidNo ratings yet
- SeminarDocument36 pagesSeminarKhadira MohammedNo ratings yet
- Ear Emergencies: Thomas Morrissey and John B. LissowayDocument11 pagesEar Emergencies: Thomas Morrissey and John B. LissowayFajriah SaraswatiNo ratings yet
- Oral and Dental Management in Children With Tetralogy of FallotDocument4 pagesOral and Dental Management in Children With Tetralogy of FallotRisyaRahmadaniNo ratings yet
- Prevention and Rehabilitation of Old Age DeafnessDocument8 pagesPrevention and Rehabilitation of Old Age DeafnessXilena HerreraNo ratings yet
- Ha - Asssessing EarsDocument6 pagesHa - Asssessing EarsKenneth Andre Batuyog TecsonNo ratings yet
- ENT - Diseases of The Inner Ear 2014Document4 pagesENT - Diseases of The Inner Ear 2014Thakoon TtsNo ratings yet
- Nikolaus Ronald Indra 4Document137 pagesNikolaus Ronald Indra 4Florence StellaNo ratings yet
- Pemicu 4 Eko Blok PenginderaanDocument59 pagesPemicu 4 Eko Blok PenginderaanEko SiswantoNo ratings yet
- Sordera SindromicaDocument8 pagesSordera SindromicaFabian Camelo OtorrinoNo ratings yet
- Hearing Impairment 1 (Document)Document10 pagesHearing Impairment 1 (Document)Jocelyn CalezaNo ratings yet
- AMBOSS Ear QuestionsDocument10 pagesAMBOSS Ear QuestionsSahil DnkNo ratings yet
- Menière 'S Disease: Mansur Amirovich Kutlubaev, Ilmari Pyykko, Todd A Hardy, Robert GürkovDocument6 pagesMenière 'S Disease: Mansur Amirovich Kutlubaev, Ilmari Pyykko, Todd A Hardy, Robert GürkovZenira PitalokaNo ratings yet
- Made By: DR Aditya RanjanDocument32 pagesMade By: DR Aditya RanjanArjun SainiNo ratings yet
- Tuberculosis Spondylitis and Pott's Curvature, Is The Most Common Site of Bone Infection in TBDocument5 pagesTuberculosis Spondylitis and Pott's Curvature, Is The Most Common Site of Bone Infection in TBAra Shian OdinerNo ratings yet
- Etiology of Hearing Loss in Adults - UpToDateDocument39 pagesEtiology of Hearing Loss in Adults - UpToDateZayNo ratings yet
- Background: Viral LabyrinthitisDocument6 pagesBackground: Viral LabyrinthitisranmiNo ratings yet
- Ear ChronicDocument44 pagesEar ChronicȜLaa AsHrafNo ratings yet
- Osteomyelitis Kronis Mandibula Pasca Ekstraksi Gigi Disertai Bell'S PalsyDocument4 pagesOsteomyelitis Kronis Mandibula Pasca Ekstraksi Gigi Disertai Bell'S PalsyDiandra Puspa WidyasariNo ratings yet
- Vestibular Neuritis and LabyrinthitisDocument18 pagesVestibular Neuritis and LabyrinthitischiquitaputriNo ratings yet
- Surgeryii: I. Benign Conditions of The Head and NeckDocument13 pagesSurgeryii: I. Benign Conditions of The Head and NeckALIMBOYOGUEN RexorNo ratings yet
- Congenital Malformations 14 MicrognathiaDocument4 pagesCongenital Malformations 14 MicrognathiaAhmed H. Ali ElbestaweyNo ratings yet
- Referat OsteomielitisDocument22 pagesReferat OsteomielitisDexel Putra Simbolon100% (1)
- Suddensnhl 160220190525Document80 pagesSuddensnhl 160220190525mariahovhannisyanNo ratings yet
- 6 OsteomyelitisDocument29 pages6 OsteomyelitisMohammed AshrefNo ratings yet
- Matsy CytoDocument7 pagesMatsy CytoDarem SoNo ratings yet
- Hearing Loss in Children - Etiology - UpToDateDocument39 pagesHearing Loss in Children - Etiology - UpToDateAlexander AdrielNo ratings yet
- Case Report Acute Coalescent MastoiditisDocument6 pagesCase Report Acute Coalescent MastoiditisWidi Yuli HariantoNo ratings yet
- Meniere's DiseaseDocument16 pagesMeniere's DiseaseKarina BundaNo ratings yet
- How Can We Diagnose and Treat Osteomyelitis of The Jaws As Early As PossibleDocument11 pagesHow Can We Diagnose and Treat Osteomyelitis of The Jaws As Early As Possiblebucomaxilofacial.hfiNo ratings yet
- Tinnitus-Diagnosis and Treatment OptionsDocument7 pagesTinnitus-Diagnosis and Treatment OptionserikafebriyanarNo ratings yet
- Hearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganDocument5 pagesHearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganMANGKAGENo ratings yet
- The Prevalence of Odontogenic Maxillary Osteitis at The 2rr2imbh89Document5 pagesThe Prevalence of Odontogenic Maxillary Osteitis at The 2rr2imbh89Johatan YanangomezNo ratings yet
- Greco 2014 ArticolDocument9 pagesGreco 2014 ArticolSabina BădilăNo ratings yet
- 03 - Pulp Diseases 2022Document18 pages03 - Pulp Diseases 2022Hazem MouradNo ratings yet
- Ocular Manifestations of Tuberculosis: SciencedirectDocument8 pagesOcular Manifestations of Tuberculosis: SciencedirectBagus Putra KurniawanNo ratings yet
- 2 5420394524511833795 PDFDocument232 pages2 5420394524511833795 PDFعبدالرحمن عبدالسلام ذنون المصريNo ratings yet
- Presentation Otitis ExternaDocument24 pagesPresentation Otitis ExternaRichard GunawanNo ratings yet
- Sensory ImpairmentDocument8 pagesSensory Impairmentadan oladiveNo ratings yet
- Noise-Induced Hearing Loss: Indian Journal of Otology December 2014Document4 pagesNoise-Induced Hearing Loss: Indian Journal of Otology December 2014مهيمن الابراهيميNo ratings yet
- Otitis Externa: DR Emma DicksonDocument7 pagesOtitis Externa: DR Emma DicksondevNo ratings yet
- Public Health Competencies HandbookDocument33 pagesPublic Health Competencies Handbookapi-556450573No ratings yet
- Long Term MemoryDocument4 pagesLong Term MemoryCamelia UrsanNo ratings yet
- WPC AssignmentDocument2 pagesWPC AssignmentPragya SinghNo ratings yet
- TamifluDocument210 pagesTamifluBogdan NeamtuNo ratings yet
- School Form 8 SF8 Learner Basic Health and Nutrition ReportDocument10 pagesSchool Form 8 SF8 Learner Basic Health and Nutrition ReportRey Moca100% (1)
- A History of Britain 1945 Through Brexit Jeremy Black Full ChapterDocument51 pagesA History of Britain 1945 Through Brexit Jeremy Black Full Chapteralice.cousin115100% (18)
- BMI CalculatorDocument1 pageBMI CalculatorchandrimaNo ratings yet
- Nutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 InfectionDocument13 pagesNutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 Infectionmmbire@gmail.comNo ratings yet
- The Role of The Microbiota-Gut-Brain Axis in Neuropsychiatric DisordersDocument13 pagesThe Role of The Microbiota-Gut-Brain Axis in Neuropsychiatric DisordersKalilNo ratings yet
- Dissociative BehaviorDocument5 pagesDissociative BehaviorDump AccNo ratings yet
- Fundamental of NursingDocument9 pagesFundamental of NursingDr-Marudhar MarudharNo ratings yet
- Test Bank For Clinical Application of Mechanical Ventilation 4th Edition Chang Isbn 10 1111539588 Isbn 13 9781111539580Document6 pagesTest Bank For Clinical Application of Mechanical Ventilation 4th Edition Chang Isbn 10 1111539588 Isbn 13 9781111539580Reed Nuss100% (35)
- All FormulasDocument3 pagesAll FormulasKevin Apeles100% (1)
- MDS ThesisDocument157 pagesMDS ThesisOmneya M. ElkadiNo ratings yet
- Pregabalin Hospital PharmacyDocument16 pagesPregabalin Hospital PharmacyadityaNo ratings yet
- Pe103-Course-Guide-And-Module-Sem. 2022-2023Document55 pagesPe103-Course-Guide-And-Module-Sem. 2022-2023Thomas Danjo ManulatNo ratings yet
- Test Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordDocument9 pagesTest Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordJack WittersNo ratings yet
- 10.1002@lary.28626 EngDocument7 pages10.1002@lary.28626 EngRima Fairuuz PutriNo ratings yet
- Anxiety 2Document11 pagesAnxiety 2tela teliNo ratings yet
- Cranial NervesDocument5 pagesCranial NervesTHE BLINKNo ratings yet
- 1ero Bachillerato Semana 3 y 4 Engish 2020-2021Document2 pages1ero Bachillerato Semana 3 y 4 Engish 2020-2021Andres Andy MamallactaNo ratings yet
- Anthropometric MeasurementsDocument11 pagesAnthropometric MeasurementsKinjal SharmaNo ratings yet
- Challenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesDocument3 pagesChallenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesHerald Scholarly Open AccessNo ratings yet
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet