You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tabulation SheetDocument1 pageTabulation SheetKresta Benigno100% (2)
- Letter of RecomendationDocument2 pagesLetter of RecomendationJorge Luis Sánchez Alarcón100% (1)
- DRRM CCAM PlanDocument2 pagesDRRM CCAM PlanKresta Benigno100% (3)
- Sample Action Research in MathDocument12 pagesSample Action Research in MathKresta BenignoNo ratings yet
- Acute Pain NCPDocument2 pagesAcute Pain NCPfaye-pamatmat-257080% (5)
- Serotonin SyndromeDocument19 pagesSerotonin SyndromeNur Atiqah Mohd AzliNo ratings yet
- Medical Oncology JNR HandbookDocument50 pagesMedical Oncology JNR Handbookhmudeveloper100% (1)
- Kinder: Jawod Elementary School Class ScheduleDocument7 pagesKinder: Jawod Elementary School Class ScheduleKresta BenignoNo ratings yet
- School Coordination GroupDocument8 pagesSchool Coordination GroupKresta BenignoNo ratings yet
- LOCATOR SLIP (Permission To Leave Station)Document8 pagesLOCATOR SLIP (Permission To Leave Station)Kresta BenignoNo ratings yet
- Travel Certificate: Barangay BucayaDocument5 pagesTravel Certificate: Barangay BucayaKresta BenignoNo ratings yet
- The Key To Effective Classroom ManagementDocument23 pagesThe Key To Effective Classroom ManagementKresta BenignoNo ratings yet
- JawodES Contingency PlanDocument19 pagesJawodES Contingency PlanKresta BenignoNo ratings yet
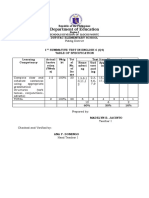
- Quarter 4, First Summative Test in All Subjects (With Tos and Answer KeyDocument45 pagesQuarter 4, First Summative Test in All Subjects (With Tos and Answer KeyKresta BenignoNo ratings yet
- Social and Emotional LearningDocument1 pageSocial and Emotional LearningKresta BenignoNo ratings yet
- 2nd Quarter Narrative NSED ReportDocument3 pages2nd Quarter Narrative NSED ReportKresta Benigno100% (1)
- Stop! Burn Out, Use Your Time Wisely: Ecclesiastes 3:1-2Document19 pagesStop! Burn Out, Use Your Time Wisely: Ecclesiastes 3:1-2Kresta BenignoNo ratings yet
- Remedial ListDocument1 pageRemedial ListKresta BenignoNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- CERTIFICATES by SavDocument11 pagesCERTIFICATES by SavKresta BenignoNo ratings yet
- Brigada PangsolicitDocument1 pageBrigada PangsolicitKresta BenignoNo ratings yet
- Instructions For The Diagnosticwindow Cards in Mathematics For Elementary GradesDocument8 pagesInstructions For The Diagnosticwindow Cards in Mathematics For Elementary GradesKresta Benigno100% (2)
- NCP and Drug StudyDocument11 pagesNCP and Drug StudyTonio PagaoNo ratings yet
- Lung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Document53 pagesLung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Mr. IncognitoNo ratings yet
- My Trip To and Through SwitchwordsDocument3 pagesMy Trip To and Through SwitchwordssolmazbaharyNo ratings yet
- Personal BoundariesDocument4 pagesPersonal Boundariesscribdreaderplus75% (4)
- Carmin WentworthDocument4 pagesCarmin Wentworthapi-356549360No ratings yet
- ATI DRUG TABLES Module4 Respiratory Glucocorticoids InhalationDocument1 pageATI DRUG TABLES Module4 Respiratory Glucocorticoids InhalationnoeyeshaveseenNo ratings yet
- List-European-Union-Reference-Dates-Frequency-Submission-Periodic-Safety-Update-Reports - en (2) UpdatedDocument40 pagesList-European-Union-Reference-Dates-Frequency-Submission-Periodic-Safety-Update-Reports - en (2) UpdatedMai MostafaNo ratings yet
- TG-43 ArDocument68 pagesTG-43 ArCecilia Querebalu Garcia0% (1)
- Homeopathic Materia Medica by Farrington Causticum (Caust) : Lecture Lxxi Lecture LxxiiDocument7 pagesHomeopathic Materia Medica by Farrington Causticum (Caust) : Lecture Lxxi Lecture LxxiimyoxusNo ratings yet
- Biophysics 102 Lecture 3 1Document13 pagesBiophysics 102 Lecture 3 1Nada Atef KoraitemNo ratings yet
- Aplastic AnemiaDocument3 pagesAplastic AnemiaFrancis JuneNo ratings yet
- Evidence Base Update For Autism Spectrum DisorderDocument27 pagesEvidence Base Update For Autism Spectrum DisorderLINDA MARiA NATALY FeLIX PEREZNo ratings yet
- Severe and Multiple DisabilitiesDocument18 pagesSevere and Multiple DisabilitiesKavi Rehabian100% (1)
- MBRDocument9 pagesMBRAuspicious MuthuNo ratings yet
- A Fireman and His Rescue Dog On A MissionDocument3 pagesA Fireman and His Rescue Dog On A MissionPR.comNo ratings yet
- Med-Fit 3: Instruction Manual Betriebsanleitung Manuel D'instructionDocument52 pagesMed-Fit 3: Instruction Manual Betriebsanleitung Manuel D'instructionCarlos ParraNo ratings yet
- ADHD Parent Questionnaire PDFDocument4 pagesADHD Parent Questionnaire PDFklichtNo ratings yet
- Slide Ortho Tibia and FibulaDocument25 pagesSlide Ortho Tibia and Fibulaleonard0% (1)
- Julie Reznicek, Paul W. Perdue, JR., Gonzalo Bearman - Musculoskeletal Infections - A Clinical Case Book-Springer (2020)Document230 pagesJulie Reznicek, Paul W. Perdue, JR., Gonzalo Bearman - Musculoskeletal Infections - A Clinical Case Book-Springer (2020)Medicine Essentials SimplifiedNo ratings yet
- Interesting Case FinalDocument33 pagesInteresting Case Finalazenith dumlaoNo ratings yet
- Diabetes EvaluationDocument3 pagesDiabetes Evaluatione-MedTools100% (3)
- Cayman Islands National Youth Policy September 2000Document111 pagesCayman Islands National Youth Policy September 2000Kyler GreenwayNo ratings yet
- Fibromyalgia PDFDocument5 pagesFibromyalgia PDFYalile TurkaNo ratings yet
- DIALOGUE AND EXPERIMENT by Peter PhilippsonDocument6 pagesDIALOGUE AND EXPERIMENT by Peter PhilippsonMariana BorodeaNo ratings yet
- Book Reviews: Trigger Points and Muscle Chains in OsteopathyDocument4 pagesBook Reviews: Trigger Points and Muscle Chains in OsteopathyConstanza López MillerNo ratings yet
- White Lesion 7Document114 pagesWhite Lesion 7Samina TarikNo ratings yet