You might also like
- Ethics in Health Services Management, Sixth Edition (Excerpt)Document12 pagesEthics in Health Services Management, Sixth Edition (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.57% (7)
- Example - NURS FPX 4050 Assessment 2 (Safe Assign 22Document7 pagesExample - NURS FPX 4050 Assessment 2 (Safe Assign 22akko aliNo ratings yet
- Chapter 176Document13 pagesChapter 176Intan Sanditiya AlifNo ratings yet
- Module 6 - Principle of Cooperation in Evil SupplementalDocument5 pagesModule 6 - Principle of Cooperation in Evil SupplementalcyrhenmieNo ratings yet
- The Principle of CooperationDocument2 pagesThe Principle of CooperationRia Mallane TioNo ratings yet
- Isip, Erwin Gabriel C.Document6 pagesIsip, Erwin Gabriel C.Erwin IsipNo ratings yet
- Appropriation of EvilDocument34 pagesAppropriation of EvilThằng ThấyNo ratings yet
- Is Homosexuality SexualityDocument12 pagesIs Homosexuality SexualityLCLibraryNo ratings yet
- Basic Ethical Principles 1 StewardshipDocument8 pagesBasic Ethical Principles 1 StewardshipGlizzle MacaraegNo ratings yet
- Basic Ethical Principles 1. StewardshipDocument5 pagesBasic Ethical Principles 1. Stewardshipmitsuki_sylph71% (7)
- Bioethics PremidDocument16 pagesBioethics Premidfatimie rozinne amilbangsaNo ratings yet
- Local Media7197619751455914340Document61 pagesLocal Media7197619751455914340PABLO, JACKSON P.No ratings yet
- J Med Ethics 1999 Kottow 340 3Document5 pagesJ Med Ethics 1999 Kottow 340 3Pier Paolo Dal MonteNo ratings yet
- Ethics To TheologyDocument6 pagesEthics To Theologygem005No ratings yet
- Sample Thesis RH BillDocument8 pagesSample Thesis RH Billangelahaysnorman100% (2)
- 1984 - Patients' Ethical Obligation For Their HealthDocument5 pages1984 - Patients' Ethical Obligation For Their HealthDaniel MeloNo ratings yet
- Lx83vu8jl - BASIC ETHICAL PRINCIPLES - BIOETHICSDocument19 pagesLx83vu8jl - BASIC ETHICAL PRINCIPLES - BIOETHICSEvelyn MedinaNo ratings yet
- Miedema 1993Document11 pagesMiedema 1993mariana alvarezNo ratings yet
- Course: UU200 - Ethics and Governance Name: Wayne Atu Luciano Id: s11150128 Assignment 3 - Research Essay Campus: LautokaDocument7 pagesCourse: UU200 - Ethics and Governance Name: Wayne Atu Luciano Id: s11150128 Assignment 3 - Research Essay Campus: LautokaWayne LucianoNo ratings yet
- Notes For ArticleDocument5 pagesNotes For ArticleRamil Andrea BoybantingNo ratings yet
- Communicating About HealthsDocument53 pagesCommunicating About HealthsdoetphipgoattuynhNo ratings yet
- An Interactive Model of Clinical-Ethical Decision MakingDocument14 pagesAn Interactive Model of Clinical-Ethical Decision MakingMuhammad Na'im100% (7)
- Chapter Iv-Medical Negligence 4.1 Medical Negligence Statement of The ProblemDocument9 pagesChapter Iv-Medical Negligence 4.1 Medical Negligence Statement of The ProblemKranthi TalluriNo ratings yet
- 16th Bienial Nursing Leaders ConferenceDocument25 pages16th Bienial Nursing Leaders ConferenceabdulNo ratings yet
- Teori Etika KeperawatanDocument19 pagesTeori Etika Keperawatandwidui93No ratings yet
- PhilosophyDocument6 pagesPhilosophyjamilasaeed777No ratings yet
- Joanne Tomas Health Ethics BSN 2-2docxDocument3 pagesJoanne Tomas Health Ethics BSN 2-2docxBSN 22 Joanne TomasNo ratings yet
- The Principle of Autonomy: Four Fundamental Ethical PrinciplesDocument7 pagesThe Principle of Autonomy: Four Fundamental Ethical PrinciplesROMELA MAQUILINGNo ratings yet
- Healthcare Ethics l1Document4 pagesHealthcare Ethics l122-55921No ratings yet
- Basic Ethical Principles 1. StewardshipDocument2 pagesBasic Ethical Principles 1. StewardshipDiana Laura LeiNo ratings yet
- Elvira BoiethicsDocument2 pagesElvira BoiethicsElvira GumiNo ratings yet
- 3 Ethico-MoralDocument23 pages3 Ethico-MoralBethany Dedray GilladogaNo ratings yet
- Common Factors + DefinitionDocument8 pagesCommon Factors + DefinitionVal AvivNo ratings yet
- Bærøe & Baltussen, 2014Document15 pagesBærøe & Baltussen, 2014Pantelis TsavalasNo ratings yet
- Act4181 Induvidual AssignmentDocument6 pagesAct4181 Induvidual AssignmentMuadz KamaruddinNo ratings yet
- Sources EthicsDocument7 pagesSources Ethicsapi-548466185No ratings yet
- Guevarra Eunice B. - Chapter 3 Decision Making in Value Issues and Private LawDocument5 pagesGuevarra Eunice B. - Chapter 3 Decision Making in Value Issues and Private LawGUEVARRA EUNICE B.No ratings yet
- Principles of BioethicsDocument7 pagesPrinciples of BioethicsNuronnisah Kalinggalan PadjiriNo ratings yet
- CW Ethics PaperDocument6 pagesCW Ethics Paperapi-368504287No ratings yet
- Healthcare ProfessionDocument7 pagesHealthcare ProfessionAndriaNo ratings yet
- Utilitarianism Versus Kant Case Three: Confidentiality: by Linda S. NeffDocument10 pagesUtilitarianism Versus Kant Case Three: Confidentiality: by Linda S. NeffJaymie DioNo ratings yet
- The Reason Is ThatDocument2 pagesThe Reason Is ThatNathanNo ratings yet
- Acta Psychiatrica Scandinavica Volume 101 Issue 399 2000 (Doi 10.1111 - j.0902-4441.2000.007s020 (Dash) 16.x) G. Høyer - On The JustificationDocument7 pagesActa Psychiatrica Scandinavica Volume 101 Issue 399 2000 (Doi 10.1111 - j.0902-4441.2000.007s020 (Dash) 16.x) G. Høyer - On The JustificationMariusNo ratings yet
- Mindanao State Univesity - Marawi City: College of Health SciencesDocument3 pagesMindanao State Univesity - Marawi City: College of Health SciencesJULIA MARIE ALMORADONo ratings yet
- Principles of BioethicsDocument5 pagesPrinciples of Bioethicsbanyenye25No ratings yet
- Ethical Issues in Counselling N Psychotherapy PracticeDocument257 pagesEthical Issues in Counselling N Psychotherapy Practicesumukh.knNo ratings yet
- (Book Review Of) - em - Ethics and Regulation of Clinical ResearchDocument3 pages(Book Review Of) - em - Ethics and Regulation of Clinical ResearchmghaseghNo ratings yet
- Ethics and Law for Neurosciences Clinicians: Foundations and Evolving ChallengesFrom EverandEthics and Law for Neurosciences Clinicians: Foundations and Evolving ChallengesNo ratings yet
- Week 10 - Continuing Education Programs On Ethico-Moral Practice in NursingDocument4 pagesWeek 10 - Continuing Education Programs On Ethico-Moral Practice in NursingAmori Studios0% (1)
- RH BillDocument2 pagesRH BillJalden JadenNo ratings yet
- SHeS Bioethics Reading Material 1Document4 pagesSHeS Bioethics Reading Material 1Mel Ligen DIANANo ratings yet
- Wampold, B. 2015. How Important Are The Common Factors in Psychotherapy. An UpdateDocument8 pagesWampold, B. 2015. How Important Are The Common Factors in Psychotherapy. An UpdateMARIO APPELIUS SANHUEZANo ratings yet
- Gabonada, Anthony, GEN SCI BDocument3 pagesGabonada, Anthony, GEN SCI BAntonio VallejosNo ratings yet
- BioethicsDocument6 pagesBioethicsDiana Laura LeiNo ratings yet
- 25.3.shaw Web PDFDocument32 pages25.3.shaw Web PDFJournal of Law, Information & ScienceNo ratings yet
- The Nursing Code of Ethics Its Value, Its HistoryDocument14 pagesThe Nursing Code of Ethics Its Value, Its HistoryalifahNo ratings yet
- Journal Article ResearchDocument23 pagesJournal Article ResearchRamil Andrea BoybantingNo ratings yet
- The Role of Ethical Principles in Health Care and The Implications For Ethical CodesDocument6 pagesThe Role of Ethical Principles in Health Care and The Implications For Ethical CodesNewfaceNo ratings yet
- Basic Ethical PrinciplesDocument3 pagesBasic Ethical Principlesms_pianistNo ratings yet
- Ds 42 Upgrade enDocument118 pagesDs 42 Upgrade enJaviera OrellanaNo ratings yet
- 3 Disability ModelsDocument28 pages3 Disability ModelszainbNo ratings yet
- Chapter 5 & 6Document28 pagesChapter 5 & 6劉力僑 LIU,LI-CIAO E34116324No ratings yet
- Jaltarang Instruments ShreyaDocument24 pagesJaltarang Instruments ShreyaKaushal DidwaniaNo ratings yet
- Leif Eriksson-Annotated BibDocument7 pagesLeif Eriksson-Annotated Bibapi-308958050No ratings yet
- Presentations 2023Document6 pagesPresentations 2023Tawanda MatongeraNo ratings yet
- Corporation PDFDocument8 pagesCorporation PDFKAMALINo ratings yet
- Competency Checklist For CparDocument2 pagesCompetency Checklist For CparChristine Marie A Llanera-CadalloNo ratings yet
- 7541678Document11 pages7541678CaitlinNo ratings yet
- Sources of Islamic LawDocument7 pagesSources of Islamic LawTayyab H. HashmiNo ratings yet
- 26Document7 pages26Rinandar MusliminNo ratings yet
- Chapter 4 - Wilhelm Wundt and The Founding of Psychology: Dr. Nancy AlvaradoDocument27 pagesChapter 4 - Wilhelm Wundt and The Founding of Psychology: Dr. Nancy AlvaradoAdalene SalesNo ratings yet
- 1 PBDocument15 pages1 PBKhoirunnisaNo ratings yet
- MPS and Item AnalysisDocument177 pagesMPS and Item AnalysisMary Ann Palima80% (5)
- TMC451 Sample - Skema JWPDocument2 pagesTMC451 Sample - Skema JWPraihana abdulkarimNo ratings yet
- First Motion For Declaratory JudgmentDocument15 pagesFirst Motion For Declaratory JudgmentRobert Davidson, M.D., Ph.D.100% (2)
- The Life of SolomonDocument6 pagesThe Life of SolomonReste Marion MartizanoNo ratings yet
- Ways To Stimulate Your ChildDocument2 pagesWays To Stimulate Your ChildRommel RomuloNo ratings yet
- Daftar PustakaDocument11 pagesDaftar PustakaHilyaNo ratings yet
- Solution of IWTDocument6 pagesSolution of IWTreetikaNo ratings yet
- ECS 202301 Lecture 5 2Document35 pagesECS 202301 Lecture 5 2Rhinndhi SakthyvelNo ratings yet
- Rahail's ResumeDocument3 pagesRahail's ResumeRahailSalamatNo ratings yet
- Theory Matrix 2Document2 pagesTheory Matrix 2api-654837218No ratings yet
- 2016 GP Y5 Infopack - Media + Social Issues - FINAL PDFDocument104 pages2016 GP Y5 Infopack - Media + Social Issues - FINAL PDFMelissaNo ratings yet
- 6QQMN969 Module OutlineDocument4 pages6QQMN969 Module OutlineyuvrajwilsonNo ratings yet
- Picot (TT) Evidenced Based Practice: What Does Picot Stands For?Document35 pagesPicot (TT) Evidenced Based Practice: What Does Picot Stands For?angel sychingNo ratings yet
- Chapter 11 - LossesDocument20 pagesChapter 11 - LossesMutong ZhengNo ratings yet
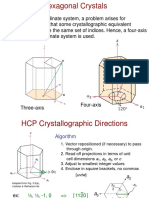
- Chap3.3 HexCrystal DirectionsDocument6 pagesChap3.3 HexCrystal DirectionsJeonghun LeeNo ratings yet
- Overseas Road Note 04 PDFDocument44 pagesOverseas Road Note 04 PDFbala subramanyamNo ratings yet