You might also like
- Ventilator Associated Pneumonia: Incidence, Profile and Outcome in Pediatric Intensive Care Unit of Tertiary Care CentreDocument5 pagesVentilator Associated Pneumonia: Incidence, Profile and Outcome in Pediatric Intensive Care Unit of Tertiary Care CentreJoaquín SosaNo ratings yet
- 4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestDocument18 pages4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestGhimpu DanielaNo ratings yet
- 5882-PDF Galley-38159-1-10-20201216Document5 pages5882-PDF Galley-38159-1-10-20201216MF SNo ratings yet
- Mortalidad PardsDocument9 pagesMortalidad PardsBarbara Seminario RamirezNo ratings yet
- 5754-Article Text-43741-3-10-20220520Document18 pages5754-Article Text-43741-3-10-20220520Ricardo TanNo ratings yet
- Song Zan 2019 Hypoalbuminemia A Novel Prognostic Factor ForDocument9 pagesSong Zan 2019 Hypoalbuminemia A Novel Prognostic Factor ForRazan RabiNo ratings yet
- Clinical Characteristics of Critically-Ill Heat Stroke PopulationDocument6 pagesClinical Characteristics of Critically-Ill Heat Stroke PopulationijasrjournalNo ratings yet
- Clinical Characteristics of Critically-Ill Heat Stroke PopulationDocument6 pagesClinical Characteristics of Critically-Ill Heat Stroke PopulationijasrjournalNo ratings yet
- Diagnostics 10 00382Document20 pagesDiagnostics 10 00382Harpreet SinghNo ratings yet
- Initial Hemodynamic Profiles of Children with Dengue Shock SyndromeDocument7 pagesInitial Hemodynamic Profiles of Children with Dengue Shock SyndromeEly macNo ratings yet
- Early Risk Factors For Mortality in Children With SeizureDocument6 pagesEarly Risk Factors For Mortality in Children With Seizurehilman lesmanaNo ratings yet
- Clinical Characteristics and Treatment of Severe Encephalitis Associated With Neurogenic Pulmonary Edema Caused by Enterovirus 71 in ChinaDocument6 pagesClinical Characteristics and Treatment of Severe Encephalitis Associated With Neurogenic Pulmonary Edema Caused by Enterovirus 71 in ChinanurulmaulidyahidayatNo ratings yet
- Increased Fluid Administration in The First TH Ree Hours of Sepsis Resuscitation Is Associated With Reduced MortalityDocument8 pagesIncreased Fluid Administration in The First TH Ree Hours of Sepsis Resuscitation Is Associated With Reduced MortalityAzmachamberAzmacareNo ratings yet
- Identificacion Choque Cardiogenico ERDocument9 pagesIdentificacion Choque Cardiogenico ERZai RojasNo ratings yet
- Strokeaha 118 021301Document6 pagesStrokeaha 118 021301Rahma Nur AmeliaNo ratings yet
- Endocarditis in Children With Congenital Heart DiseaseDocument3 pagesEndocarditis in Children With Congenital Heart DiseaseDewi PrasetiaNo ratings yet
- Epidemiology and Clinical Profile of PIMS-TS. Dhanalakshmi Ind Pediatr Aug 2020Document10 pagesEpidemiology and Clinical Profile of PIMS-TS. Dhanalakshmi Ind Pediatr Aug 2020Bala RamachandranNo ratings yet
- Clinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiaDocument6 pagesClinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiamariaprincesitaNo ratings yet
- Rapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicDocument3 pagesRapid Training of Healthcare Staff For Protected Cardiopulmonary Resuscitation in The COVID-19 PandemicRicardo BarreraNo ratings yet
- Ischemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesDocument20 pagesIschemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesIJAR JOURNALNo ratings yet
- 10.1007@s11739 019 02196 ZDocument10 pages10.1007@s11739 019 02196 ZMaharani Sari NastitiNo ratings yet
- Nursing Workload Associated With Fever in The General Intensive Care UnitDocument13 pagesNursing Workload Associated With Fever in The General Intensive Care UnitAyuq NurasisNo ratings yet
- P0581 548 Risk Factors of Severity of Dengue.639Document1 pageP0581 548 Risk Factors of Severity of Dengue.639Hendri HariyantoNo ratings yet
- 1 s2.0 S003139551730069XDocument12 pages1 s2.0 S003139551730069XclaudiaNo ratings yet
- Elaxim ResearchDocument6 pagesElaxim ResearchMayukh BanerjeeNo ratings yet
- 1-s2.0-S1525505013004186 TUGAS INDAH-mainDocument5 pages1-s2.0-S1525505013004186 TUGAS INDAH-mainRendi Er PratamaNo ratings yet
- Clinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapyDocument10 pagesClinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapySuci ZahraniNo ratings yet
- Diagnostic Approach for PancytopeniaDocument7 pagesDiagnostic Approach for PancytopeniaDani BelloNo ratings yet
- Epidemiology of Pediatric Acute Encephalitis/Encephalopathy in JapanDocument7 pagesEpidemiology of Pediatric Acute Encephalitis/Encephalopathy in Japaneko andryNo ratings yet
- GuiasddddDocument10 pagesGuiasddddKarla CastilloNo ratings yet
- Jurnal Bhs InggrisDocument12 pagesJurnal Bhs InggrisnurulNo ratings yet
- LANCET 12-Citicolina (Somazina) en Tratamiento de Ictus IsquemicoDocument9 pagesLANCET 12-Citicolina (Somazina) en Tratamiento de Ictus IsquemicorhymescsfNo ratings yet
- BMC NeurologyDocument8 pagesBMC NeurologyTarun MathurNo ratings yet
- Psychological Response COVID Renal TXDocument5 pagesPsychological Response COVID Renal TXdrshhagarNo ratings yet
- Clinical OncologyDocument8 pagesClinical OncologyHector VillaseñorNo ratings yet
- Cardiac Interventions in Neonates WiDocument11 pagesCardiac Interventions in Neonates WiimNo ratings yet
- Research Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryDocument5 pagesResearch Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryAyu Septiari ArtatiNo ratings yet
- Typhoid JournalDocument7 pagesTyphoid JournalRegina AyediaNo ratings yet
- Art:10.1186/s13054 016 1252 2Document9 pagesArt:10.1186/s13054 016 1252 2IsnaNo ratings yet
- Prospective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in a Tertiary Care Pediatric SettingDocument7 pagesProspective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in a Tertiary Care Pediatric SettingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Early ViewDocument34 pagesEarly Viewyesid urregoNo ratings yet
- Evaluation_of_clinical_spectrum_and_risk_factors_iDocument9 pagesEvaluation_of_clinical_spectrum_and_risk_factors_imeenakshi.r.agrawalNo ratings yet
- Intraoperative Cardiac Arrests in Adults.20Document9 pagesIntraoperative Cardiac Arrests in Adults.20Werner Ruben Granados NavarroNo ratings yet
- 2022 - After Nectarine How Should We Provide Anesthesia.14Document6 pages2022 - After Nectarine How Should We Provide Anesthesia.14Pamela Mamani FloresNo ratings yet
- Stroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeDocument7 pagesStroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeAnonymous XO9RqHhOgiNo ratings yet
- Diagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockDocument7 pagesDiagnosis, Management, and Outcomes of Patients With Syncope and Bundle Branch BlockPaul CalbureanNo ratings yet
- Pediatric Acute Asthma Scoring Systems: A Systematic Review and Survey of UK PracticeDocument9 pagesPediatric Acute Asthma Scoring Systems: A Systematic Review and Survey of UK PracticeM Tevfik ÇeviriciNo ratings yet
- Non Traumatic ComaDocument8 pagesNon Traumatic ComasuyalamitNo ratings yet
- 3. khemani2009Document7 pages3. khemani2009Dwi Putri SekariniNo ratings yet
- Scrub Typhus Meningitis in ChildrenDocument6 pagesScrub Typhus Meningitis in Childrenandrian dwiNo ratings yet
- INTRODUCTIONDocument8 pagesINTRODUCTIONPharmanic By Ruttaba FatimaNo ratings yet
- Clinical Audit On One Hour Sepsis Bundle in Our HospitalDocument2 pagesClinical Audit On One Hour Sepsis Bundle in Our HospitalAnonymous lAfk9gNPNo ratings yet
- Can Lactate Clearance Predict Mortality in Critically Ill Children?Document6 pagesCan Lactate Clearance Predict Mortality in Critically Ill Children?Sam Aguilar FigueroaNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- TBC y Shock SepticoDocument9 pagesTBC y Shock Septicogiseladelarosa2006No ratings yet
- Concise Report: Efficacy and Tolerance of Infliximab in Refractory Takayasu Arteritis: French Multicentre StudyDocument5 pagesConcise Report: Efficacy and Tolerance of Infliximab in Refractory Takayasu Arteritis: French Multicentre StudyMikhail PisarevNo ratings yet
- Aborto septico Lanari-USA ICM 2004Document6 pagesAborto septico Lanari-USA ICM 2004pastorizaariana25No ratings yet
- 44 Journals ACNRJF11Document3 pages44 Journals ACNRJF11Airin QueNo ratings yet
- Ijcmcr RW 00608Document4 pagesIjcmcr RW 00608childicuNo ratings yet
- Heart Clinical Case by SlidesgoDocument53 pagesHeart Clinical Case by SlidesgoUlfa Sari Al-BahmiNo ratings yet
- Dampak Covid-19 terhadap Perubahan Psikologis, Sosial dan Ekonomi Pasien Covid-19Document14 pagesDampak Covid-19 terhadap Perubahan Psikologis, Sosial dan Ekonomi Pasien Covid-19IsnatainiNo ratings yet
- Dzakiyah Nurul IsraDocument1 pageDzakiyah Nurul IsraUlfa Sari Al-BahmiNo ratings yet
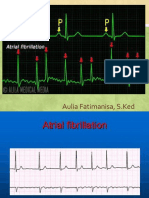
- Atrial FibrilasiDocument6 pagesAtrial FibrilasiUlfa Sari Al-BahmiNo ratings yet
- 8.8.2017 - Fracture of FemurDocument57 pages8.8.2017 - Fracture of FemurUlfa Sari Al-BahmiNo ratings yet
- BS BuzzDocument10 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Modals of Suggestion HomeworkDocument2 pagesModals of Suggestion HomeworkmateoNo ratings yet
- Practice Sheet Session 2 - 2021 - Student SheetDocument2 pagesPractice Sheet Session 2 - 2021 - Student SheetAlisa SayNo ratings yet
- Professional Hypnotherapist Diploma For Stress CourseDocument53 pagesProfessional Hypnotherapist Diploma For Stress CourseLuis Del Valle Torregrosa100% (1)
- Selcoperm SES 125-2000 Electrochlorinator: Installation and Operating InstructionsDocument32 pagesSelcoperm SES 125-2000 Electrochlorinator: Installation and Operating InstructionsNorbert MeyerNo ratings yet
- RA-032739 - MASTER PLUMBER - Lucena - 2-2023Document7 pagesRA-032739 - MASTER PLUMBER - Lucena - 2-2023Bon Opeña GorobaoNo ratings yet
- A Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItDocument1 pageA Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItSanjeev Sharma100% (2)
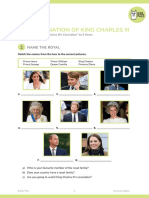
- SV The Coronation of King Charles IIIDocument9 pagesSV The Coronation of King Charles IIIMaria GromovaNo ratings yet
- Treatment Plan PortfolioDocument2 pagesTreatment Plan Portfolioapi-518560779No ratings yet
- H2S Monitor Manual - Tango TX1Document50 pagesH2S Monitor Manual - Tango TX1MattNo ratings yet
- 10 Things I Would Do If I Were A CelebrityDocument3 pages10 Things I Would Do If I Were A CelebrityAnne Marian JosephNo ratings yet
- End of Life Care GuideDocument79 pagesEnd of Life Care GuideAbcd TolibasNo ratings yet
- Flooding in Pakistan: Overview and Issues For Congress: K. Alan Kronstadt, CoordinatorDocument33 pagesFlooding in Pakistan: Overview and Issues For Congress: K. Alan Kronstadt, Coordinatorahmed shakeelNo ratings yet
- Pharmacology Course IntroductionDocument2 pagesPharmacology Course IntroductionHassen ZabalaNo ratings yet
- NGYouthSDGs PlaybookDocument50 pagesNGYouthSDGs PlaybookLaura noguesNo ratings yet
- Pediatric History Taking & Pe Simulation: Student'S Task Done Not DoneDocument8 pagesPediatric History Taking & Pe Simulation: Student'S Task Done Not DoneFrancis CervantesNo ratings yet
- Passion Project Action PlanDocument3 pagesPassion Project Action PlanMeresa W. MartinNo ratings yet
- Flow Penanganan DeviasiDocument4 pagesFlow Penanganan DeviasiGaluhNo ratings yet
- HS ConsultantDocument2 pagesHS Consultantdeeman4yahNo ratings yet
- SINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsDocument14 pagesSINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsSaquib.MahmoodNo ratings yet
- Medical Checkup PackagesDocument2 pagesMedical Checkup PackagesLia AnggitaNo ratings yet
- VA - DQA Specialist IBTCIDocument5 pagesVA - DQA Specialist IBTCIT. Woibah SuwoNo ratings yet
- Personal Values, Beliefs and AttitudesDocument10 pagesPersonal Values, Beliefs and Attitudesapi-282066793No ratings yet
- Addicted To Phones - Reading AssignmentDocument4 pagesAddicted To Phones - Reading AssignmentLilith PersephoneNo ratings yet
- Circulation and Blood 1B.1Document17 pagesCirculation and Blood 1B.1tas xoNo ratings yet
- Medical Certificate: Healthservices@lnu - Edu.phDocument3 pagesMedical Certificate: Healthservices@lnu - Edu.phNiko ChavezNo ratings yet
- Workplace Hazards and Safety PoliciesDocument4 pagesWorkplace Hazards and Safety Policiesmaya_muthNo ratings yet
- Trainee's Record Book SWBLDocument12 pagesTrainee's Record Book SWBLaaronjules100% (2)
- Guide To Dating For Autistic AdultsDocument3 pagesGuide To Dating For Autistic AdultsManasi PhanseNo ratings yet
- 2 NdresearchpaperDocument5 pages2 Ndresearchpaperapi-356685046No ratings yet