You might also like
- Genomic Biomarkers for Pharmaceutical Development: Advancing Personalized Health CareFrom EverandGenomic Biomarkers for Pharmaceutical Development: Advancing Personalized Health CareYihong YaoNo ratings yet
- PHAR Article 73597 en 1Document7 pagesPHAR Article 73597 en 1AhmadNo ratings yet
- Drug Prescribing Patterns in Elderly Patients in A Tertiary Level HospitalDocument6 pagesDrug Prescribing Patterns in Elderly Patients in A Tertiary Level Hospitalsangita sukumaranNo ratings yet
- Cost-Effective Analysis in Treating Diabetes Mellitus With ComorbidityDocument5 pagesCost-Effective Analysis in Treating Diabetes Mellitus With ComorbidityMONISH NAYARNo ratings yet
- Fphar 11 572569Document12 pagesFphar 11 572569hainguyen.htalabNo ratings yet
- Ghadah Asaad Assiri, Nada Atef Shebl, Mansour Adam Mahmoud, Nouf Aloudah, Elizabeth Grant, Hisham Aljadhey, Aziz SheikhDocument30 pagesGhadah Asaad Assiri, Nada Atef Shebl, Mansour Adam Mahmoud, Nouf Aloudah, Elizabeth Grant, Hisham Aljadhey, Aziz SheikhberlianNo ratings yet
- psychopharmacological treatment in borderlineDocument8 pagespsychopharmacological treatment in borderlineAndres MartinezNo ratings yet
- What Is The Epidemiology of MedicationDocument31 pagesWhat Is The Epidemiology of MedicationNadial uzmahNo ratings yet
- Prevalence of Eating Disorders Over The 2000-2018 PeriodDocument12 pagesPrevalence of Eating Disorders Over The 2000-2018 PeriodloloasbNo ratings yet
- Manuscript - 1716 - 12-TJNPR-2021-M200 Galley Proof CDocument6 pagesManuscript - 1716 - 12-TJNPR-2021-M200 Galley Proof CelisNo ratings yet
- Putrik 2014 - Access To RA BiologicsDocument13 pagesPutrik 2014 - Access To RA BiologicsNona Delia ChiriacNo ratings yet
- Functioning in Euthymic Patients With Bipolar Disorder: A Systematic Review and Meta-Analysis Using The Functioning Assessment Short TestDocument31 pagesFunctioning in Euthymic Patients With Bipolar Disorder: A Systematic Review and Meta-Analysis Using The Functioning Assessment Short TestMaria Von ShaftNo ratings yet
- Association of Smoking and Generalized ManifestatiDocument7 pagesAssociation of Smoking and Generalized ManifestatiA CASA CAIUNo ratings yet
- (JURNAL, Eng) Prescribing Potentially Inappropriate Medications For The Elderly According To Beers Criteria, Systematic ReviewDocument12 pages(JURNAL, Eng) Prescribing Potentially Inappropriate Medications For The Elderly According To Beers Criteria, Systematic ReviewAurellia Annisa WulandariNo ratings yet
- Adsijp - 18 220approvedDocument9 pagesAdsijp - 18 220approvedIndra HedarNo ratings yet
- JournalDocument6 pagesJournalfaithlophpeace21No ratings yet
- Donos. 2019. Accuracy of Single Molecular BiomarkersDocument31 pagesDonos. 2019. Accuracy of Single Molecular BiomarkersNikolas GunaldoNo ratings yet
- 2017-Ugo Chukwu-International Journal of Medicine and PharmacyDocument10 pages2017-Ugo Chukwu-International Journal of Medicine and PharmacyNurettin AbacıoğluNo ratings yet
- Geriatrics: Roger E. ThomasDocument44 pagesGeriatrics: Roger E. ThomasSubhash SharmaNo ratings yet
- Ventilator-Associated Pneumonia in Neonates and Children: A Systematic Analysis of Diagnostic Methods and PreventionDocument16 pagesVentilator-Associated Pneumonia in Neonates and Children: A Systematic Analysis of Diagnostic Methods and PreventionApotik ApotekNo ratings yet
- VR Tobacco 1Document6 pagesVR Tobacco 1m.r.velit.sNo ratings yet
- 10.1007@s10741 019 09890 2Document14 pages10.1007@s10741 019 09890 2Cha UchaNo ratings yet
- GERIATRIDocument7 pagesGERIATRIErza GenatrikaNo ratings yet
- Guia Practica DMI y DMIIDocument21 pagesGuia Practica DMI y DMIICamila Paz Colunche NuñezNo ratings yet
- Nihms 439055Document31 pagesNihms 439055Amalia NandiaNo ratings yet
- Ima 3Document7 pagesIma 3Nony KumalasariNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- Perceptions of Generic Medication in The General PopulationDocument9 pagesPerceptions of Generic Medication in The General PopulationVinky MariaNo ratings yet
- Medicina: Quality of Life of Patients With Arterial HypertensionDocument11 pagesMedicina: Quality of Life of Patients With Arterial Hypertensionwidya astutyloloNo ratings yet
- Ann Rheum Dis 2013 Edwards Annrheumdis 2013 203913Document10 pagesAnn Rheum Dis 2013 Edwards Annrheumdis 2013 203913rizki amaiNo ratings yet
- PORNIMADocument22 pagesPORNIMAagrawalnimisha2000No ratings yet
- (13142143 - Folia Medica) Pharmacoeconomics of Bronchial AsthmaDocument9 pages(13142143 - Folia Medica) Pharmacoeconomics of Bronchial AsthmaChristinaNo ratings yet
- Direct Costs of Parkinson's Disease in Brazil: A Case StudyDocument8 pagesDirect Costs of Parkinson's Disease in Brazil: A Case StudyIJAERS JOURNALNo ratings yet
- Pharmacological Augmentation in Unipolar DepressionDocument39 pagesPharmacological Augmentation in Unipolar DepressionSusana Pérez ReyesNo ratings yet
- Measuring Knowledge, Attitudes and Practices of Diabetes PatientsDocument9 pagesMeasuring Knowledge, Attitudes and Practices of Diabetes PatientsAGXfariNo ratings yet
- Physician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseDocument9 pagesPhysician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseratnatriaaNo ratings yet
- 673 FullDocument7 pages673 FullAq IfahNo ratings yet
- 2018 Value-in-HeDocument7 pages2018 Value-in-HeArchie CabacheteNo ratings yet
- FDV 090Document13 pagesFDV 090Pinna Agustien Andra YaniNo ratings yet
- Z Al-Roubaie_2020Document12 pagesZ Al-Roubaie_2020Kossay ZaouiNo ratings yet
- Carlozzi-14 RS Outcomes HDDocument20 pagesCarlozzi-14 RS Outcomes HDMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Knowledge and Attitudes Toward Self MedicationDocument16 pagesKnowledge and Attitudes Toward Self MedicationSophia Denella FelizardoNo ratings yet
- Automedicacion en Estudiantes de MedicinaDocument5 pagesAutomedicacion en Estudiantes de MedicinaBetzain Zahif MogollonNo ratings yet
- Aliment Pharmacol Ther - 2013 - Lacy - Functional Dyspepsia The Economic Impact To PatientsDocument8 pagesAliment Pharmacol Ther - 2013 - Lacy - Functional Dyspepsia The Economic Impact To PatientsBlytania EgaNo ratings yet
- Jurnal 5Document9 pagesJurnal 5raraNo ratings yet
- ScientificSummary Hta19570Document8 pagesScientificSummary Hta19570Anonymous hvOuCjNo ratings yet
- Effects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresDocument23 pagesEffects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresinkaNo ratings yet
- Journal 2 Surrogate Biomarkers For Monitoring Healthcare Quality For Chronic Diseases Such As Diabetes CareDocument3 pagesJournal 2 Surrogate Biomarkers For Monitoring Healthcare Quality For Chronic Diseases Such As Diabetes CareKim RuizNo ratings yet
- PROGRESS1Document11 pagesPROGRESS1Sergio TerrasaNo ratings yet
- Drug Prescribing Pattern and Prescription Error in Elderly: A Retrospective Study of Inpatient RecordDocument5 pagesDrug Prescribing Pattern and Prescription Error in Elderly: A Retrospective Study of Inpatient RecordhukamaNo ratings yet
- PRO49 DEVELOPMENT OF AN ALGORITHM TO IDENTIFY CLINICAL PROFILE - 2020 - Value inDocument1 pagePRO49 DEVELOPMENT OF AN ALGORITHM TO IDENTIFY CLINICAL PROFILE - 2020 - Value inMichael John AguilarNo ratings yet
- CGS DraftDocument63 pagesCGS DraftLuqmanul HakimNo ratings yet
- Primary Care Management of Knee OsteoarthritisDocument5 pagesPrimary Care Management of Knee Osteoarthritisသဲပို ေဖေဖNo ratings yet
- Analyses of Cross Sectional Data To Link The PEG With The Patie - 2022 - The JouDocument8 pagesAnalyses of Cross Sectional Data To Link The PEG With The Patie - 2022 - The JouFeyzullah TokgözNo ratings yet
- Comparison of Five Indices For Prediction of Adverse Outcomes inDocument7 pagesComparison of Five Indices For Prediction of Adverse Outcomes inJORGEJORGE63No ratings yet
- Health-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Document14 pagesHealth-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Alejandro Vesga VinchiraNo ratings yet
- Bipolar 5Document9 pagesBipolar 5Kenny KenNo ratings yet
- MCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaDocument11 pagesMCFARLANE - 2016 - ARD - EULAR-recommendations - FibromyalgiaTata2666No ratings yet
- Incidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisDocument15 pagesIncidence of Anorexia Nervosa in Women: A Systematic Review and Meta-AnalysisandreaNo ratings yet
- Dementia q6Document21 pagesDementia q6Rachel GabrielaNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- The Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipDocument15 pagesThe Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipmehakNo ratings yet
- Hobfoll Et Al., 2018 PDFDocument28 pagesHobfoll Et Al., 2018 PDFQundeel HaiderNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Relationship Between Corporate Governance, Corporate Sustainability and Financial PerformanceDocument21 pagesRelationship Between Corporate Governance, Corporate Sustainability and Financial PerformancemehakNo ratings yet
- Michel On 2010Document33 pagesMichel On 2010Tawsif HasanNo ratings yet
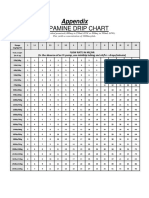
- Dopamine Drip Chart AppendixDocument1 pageDopamine Drip Chart AppendixmehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Current Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDDocument9 pagesCurrent Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDmehakNo ratings yet
- Guias Del Uso de Albumina e IgGDocument19 pagesGuias Del Uso de Albumina e IgGRonny Muñoz AcuñaNo ratings yet
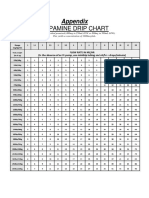
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- CVS TimetableDocument6 pagesCVS TimetableKai BinNo ratings yet
- Common ICD 10 CodesDocument2 pagesCommon ICD 10 CodesAhmadNo ratings yet
- Daftar Pustaka OpikDocument4 pagesDaftar Pustaka Opikazry shidiqNo ratings yet
- Implikasi pasien paru pada penerbanganDocument47 pagesImplikasi pasien paru pada penerbanganFebi Chyanx ElsanabiprilNo ratings yet
- INTRO TO HOME ECONOMICS LITDocument19 pagesINTRO TO HOME ECONOMICS LITClarice Gavilan100% (1)
- Case Study - IndividualDocument3 pagesCase Study - IndividualJube Kathreen ObidoNo ratings yet
- Heat Illness Prevention TrainingDocument22 pagesHeat Illness Prevention TrainingDaniel Reyes100% (1)
- Assistive Technologies For Visually Impaired MarketDocument4 pagesAssistive Technologies For Visually Impaired Marketryan2021cmrNo ratings yet
- Far Eastern University: Module 6: - Metro Manila Development Screening TestDocument18 pagesFar Eastern University: Module 6: - Metro Manila Development Screening Testjosh CNo ratings yet
- Cookbook ExcerptDocument0 pagesCookbook ExcerptchampakNo ratings yet
- The Numbered LetterDocument13 pagesThe Numbered LetterChildren's Hospice & Palliative Care CoalitionNo ratings yet
- Hypothetical HospitalDocument24 pagesHypothetical HospitalloujaneoNo ratings yet
- Posterior Uveitis HandoutDocument4 pagesPosterior Uveitis Handoutdanny wiryaNo ratings yet
- Flyadeal Low Fares Itinerary from Jeddah to DammamDocument2 pagesFlyadeal Low Fares Itinerary from Jeddah to Dammamمحمد إحسنNo ratings yet
- Sci Case ScenarioDocument3 pagesSci Case ScenarioRaymund Christopher Dela PeñaNo ratings yet
- NGL 17 40 P SP STCV - MSDS - GUS - ENDocument11 pagesNGL 17 40 P SP STCV - MSDS - GUS - ENThálitaS.PereiraNo ratings yet
- Public Assessment Report Scientific DiscussionDocument8 pagesPublic Assessment Report Scientific Discussionlhthang1990No ratings yet
- Animal Testing Essential To Medical ProgressDocument7 pagesAnimal Testing Essential To Medical ProgressLayalNo ratings yet
- FIT UK Recommendations For Injection TechniqueDocument48 pagesFIT UK Recommendations For Injection TechniqueMadeleine OchianuNo ratings yet
- Vii. Discharge Planning: Are Diarrhea, Nausea and VomitingDocument3 pagesVii. Discharge Planning: Are Diarrhea, Nausea and VomitingEköw Santiago JavierNo ratings yet
- Bachelor of Physiotherapy-Santosh Institute of Allied Health SciencesDocument10 pagesBachelor of Physiotherapy-Santosh Institute of Allied Health SciencesSantosh Institute of Allied Health SciencesNo ratings yet
- Sosialisasi E-Report IKP RS Eksternal - 2021Document32 pagesSosialisasi E-Report IKP RS Eksternal - 2021Putri Arum PermatasariNo ratings yet
- Breast - DCIS.Bx 1.0.1.0.REL CAPCPDocument6 pagesBreast - DCIS.Bx 1.0.1.0.REL CAPCPkarimahihdaNo ratings yet
- PsychopathologyDocument25 pagesPsychopathologyNaveen EldoseNo ratings yet
- Unit 2:: Unpacking The SelfDocument22 pagesUnit 2:: Unpacking The SelfCharlton Benedict BernabeNo ratings yet
- 7 Main Questions About Tummy TuckDocument3 pages7 Main Questions About Tummy TuckTandon ClinicNo ratings yet
- NursestaffDocument539 pagesNursestaffRosalyn WarrenNo ratings yet
- HSE Training Plan 2024Document10 pagesHSE Training Plan 2024md rafiqueNo ratings yet
- 1 The Philippines Sam Guidelines 2015 Final Print Ready PDFDocument111 pages1 The Philippines Sam Guidelines 2015 Final Print Ready PDFFar SultanNo ratings yet
- Does Premenstrualsyndrome Induces Change in The ANSDocument1 pageDoes Premenstrualsyndrome Induces Change in The ANSSailaja NandennagariNo ratings yet