You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 100 IC CircuitsDocument34 pages100 IC CircuitselektrorwbNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Abacus & Junior Vedic Maths SyllabusDocument2 pagesAbacus & Junior Vedic Maths SyllabusDayalan ArunachalamNo ratings yet
- PDS Syncade RADocument6 pagesPDS Syncade RAKeith userNo ratings yet
- Basic SCBA: Self-Contained Breathing ApparatusDocument51 pagesBasic SCBA: Self-Contained Breathing ApparatusPaoloFregonaraNo ratings yet
- Listeria Monocytogenes Guidance On: Environmental Monitoring and Corrective Actions in At-Risk FoodsDocument35 pagesListeria Monocytogenes Guidance On: Environmental Monitoring and Corrective Actions in At-Risk FoodsGaganpreet KaurNo ratings yet
- Datasheet - 74LS283 - Somador Binário Completo de 4 BitsDocument7 pagesDatasheet - 74LS283 - Somador Binário Completo de 4 BitsLucas CarvalhoNo ratings yet
- Understanding Blow Molding: Norman C. LeeDocument11 pagesUnderstanding Blow Molding: Norman C. LeeKiran ModakNo ratings yet
- Unicast Rotary Breaker Wear Parts: Cast To Last. Designed For Hassle-Free Removal and ReplacementDocument2 pagesUnicast Rotary Breaker Wear Parts: Cast To Last. Designed For Hassle-Free Removal and ReplacementAugusto TorresNo ratings yet
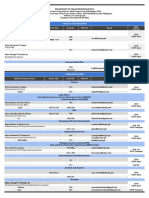
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- Mita Lifestyle Agenda ContentDocument263 pagesMita Lifestyle Agenda Contentnacentral13517No ratings yet
- Business, Government & Society: Pawan Kumar N K 12301005Document8 pagesBusiness, Government & Society: Pawan Kumar N K 12301005Pawan NkNo ratings yet
- Bubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. WilsonDocument14 pagesBubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. Wilsonliviagoncalves197271No ratings yet
- Unit 2 SignalsDocument3 pagesUnit 2 SignalsDigitallogicdlNo ratings yet
- Biomedical Uses and Applications of Inorganic Chemistry. An OverviewDocument4 pagesBiomedical Uses and Applications of Inorganic Chemistry. An OverviewHiram CruzNo ratings yet
- Theoretical Foundations of Nursing - Review MaterialDocument10 pagesTheoretical Foundations of Nursing - Review MaterialKennethNo ratings yet
- 1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroDocument80 pages1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroJayson ResultayNo ratings yet
- ActuatorsDocument24 pagesActuatorsharishcsharmaNo ratings yet
- ISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedDocument6 pagesISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedmelanitisNo ratings yet
- Installiation of Automatic Fire Sprinkler System and Design CalculationDocument8 pagesInstalliation of Automatic Fire Sprinkler System and Design CalculationSat AungNo ratings yet
- LUXEON Altilon SMDDocument25 pagesLUXEON Altilon SMDBertram PredikNo ratings yet
- QuizBowl QuestionsDocument84 pagesQuizBowl QuestionsJowel MercadoNo ratings yet
- Matter 1A Forms Properties and ChangesDocument47 pagesMatter 1A Forms Properties and ChangesSamKris Guerrero Malasaga100% (2)
- GFB V2 - VNT Boost Controller: (Part # 3009)Document2 pagesGFB V2 - VNT Boost Controller: (Part # 3009)blumng100% (1)
- Sa 387Document6 pagesSa 387ismaelarchilacastilloNo ratings yet
- Country Item Name Litre Quart Pint Nip 700 ML IndiaDocument17 pagesCountry Item Name Litre Quart Pint Nip 700 ML Indiajhol421No ratings yet
- Jotafloor: Traffic Deck SystemDocument12 pagesJotafloor: Traffic Deck SystemUnited Construction Est. TechnicalNo ratings yet
- Georgia Habitats Lesson PlansDocument5 pagesGeorgia Habitats Lesson PlansBecky BrownNo ratings yet
- Training Schedule April 2021 To March 22 - 0Document18 pagesTraining Schedule April 2021 To March 22 - 0sanrexiNo ratings yet
- H250 H250 H250 H250: Variable Area Flowmeter With 3W2 Angular Position TransmitterDocument40 pagesH250 H250 H250 H250: Variable Area Flowmeter With 3W2 Angular Position TransmitterJustine MarashanyeNo ratings yet