You might also like
- Introduction Final - EditedDocument5 pagesIntroduction Final - EditedBosco AinaniNo ratings yet
- Pengetahuan, Sikap, Dan Perilaku Wanita Hamil Terhadap Kesehatan Gigi Dan Mulut Selama Masa KehamilanDocument5 pagesPengetahuan, Sikap, Dan Perilaku Wanita Hamil Terhadap Kesehatan Gigi Dan Mulut Selama Masa KehamilanBerthi RatriyantiNo ratings yet
- Referrals For Dental Care During Pregnancy: Original ReviewDocument8 pagesReferrals For Dental Care During Pregnancy: Original ReviewxanthaineNo ratings yet
- Robison2021 Article TheImpactOfDentalInsuranceAndMDocument9 pagesRobison2021 Article TheImpactOfDentalInsuranceAndMxanthaineNo ratings yet
- Bosco Ainani 1Document5 pagesBosco Ainani 1Bosco AinaniNo ratings yet
- Dasan Ay Ake 2008Document5 pagesDasan Ay Ake 2008Elena IancuNo ratings yet
- Oral Health Coalition: Knowledge, Attitude, Practice Behaviours Among Gynaecologists and Dental PractitionersDocument8 pagesOral Health Coalition: Knowledge, Attitude, Practice Behaviours Among Gynaecologists and Dental PractitionersIndah AmaliaNo ratings yet
- How Do Dental and Prenatal Care Practitioners Perceive Dental Care During Pregnancy? Current Evidence and ImplicationsDocument10 pagesHow Do Dental and Prenatal Care Practitioners Perceive Dental Care During Pregnancy? Current Evidence and ImplicationsxanthaineNo ratings yet
- Medical Provider Promotion of Oral Health and Women's Receipt of Dental Care During PregnancyDocument13 pagesMedical Provider Promotion of Oral Health and Women's Receipt of Dental Care During PregnancyJuan Andres EspinozaNo ratings yet
- Global Issues PaperDocument5 pagesGlobal Issues Paperapi-461978440No ratings yet
- BMC Pregnancy and Childbirth: Oral and Dental Health Care Practices in Pregnant Women in Australia: A Postnatal SurveyDocument6 pagesBMC Pregnancy and Childbirth: Oral and Dental Health Care Practices in Pregnant Women in Australia: A Postnatal SurveytantriNo ratings yet
- Terapia FarmacologicaDocument13 pagesTerapia FarmacologicaDamaris RodríguezNo ratings yet
- ECC and Nursing InterventionsDocument8 pagesECC and Nursing Interventionssaima anwarNo ratings yet
- ContentServer Asp-6Document5 pagesContentServer Asp-6Estaf EmkeyzNo ratings yet
- Perilaku Ibu Hamil Dan KariesDocument22 pagesPerilaku Ibu Hamil Dan KarieshariyaniNo ratings yet
- Internet 58Document8 pagesInternet 58kriana ajiNo ratings yet
- Adpied Paper From EmailDocument17 pagesAdpied Paper From Emailapi-401213596No ratings yet
- Artikel 238Document6 pagesArtikel 238puteri asyaNo ratings yet
- Eneral: Oral Health Care During PregnancyDocument4 pagesEneral: Oral Health Care During PregnancyEstaf EmkeyzNo ratings yet
- Foreign LiteratureDocument13 pagesForeign LiteratureJm. n BelNo ratings yet
- Cunostinte GinecologiDocument6 pagesCunostinte GinecologiElena IancuNo ratings yet
- Knowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant PatientsDocument18 pagesKnowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant Patientsشبلي غرايبهNo ratings yet
- LiteratureDocument2 pagesLiteratureapi-509270104No ratings yet
- Oral Health Pregnancy ConsensusDocument12 pagesOral Health Pregnancy ConsensusAngelica SuarezNo ratings yet
- 2018 Caries and WicDocument8 pages2018 Caries and WicAlexandra Flores VillacaNo ratings yet
- Issue Focus Pregnancy and Oral Health 2-21-11Document2 pagesIssue Focus Pregnancy and Oral Health 2-21-11sonia_groff6256No ratings yet
- Knowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral HealthDocument10 pagesKnowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral HealthJuan Andres EspinozaNo ratings yet
- Oral Health in PregnancyDocument6 pagesOral Health in PregnancyTamara Al KautsarNo ratings yet
- Research Project PaperDocument6 pagesResearch Project Paperapi-369452069No ratings yet
- Balkaran20et20al Dental20treatment20during20pregnancy1Document13 pagesBalkaran20et20al Dental20treatment20during20pregnancy1Fashiona CrazeNo ratings yet
- Women'S: A Literature Review OnDocument14 pagesWomen'S: A Literature Review OnAudrey Kristina MaypaNo ratings yet
- Assessment of Knowledge, Attitude, Practice, Awareness Level of Periodontal Health and Adverse Outcomes Among Pregnant Women - A Questionnaire StudyDocument7 pagesAssessment of Knowledge, Attitude, Practice, Awareness Level of Periodontal Health and Adverse Outcomes Among Pregnant Women - A Questionnaire StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Running Head: Oral Health Care in The Geriatric Population 1Document7 pagesRunning Head: Oral Health Care in The Geriatric Population 1api-384327266No ratings yet
- Bab 1-5 Manajemen HcuDocument7 pagesBab 1-5 Manajemen Hcuretno indriyaniNo ratings yet
- Exploring The Oral Health Knowledge and Attitudes AmongDocument5 pagesExploring The Oral Health Knowledge and Attitudes AmongBosco AinaniNo ratings yet
- Ecc Lit Review - PDocument7 pagesEcc Lit Review - Papi-720438286No ratings yet
- Community Health Adpie ProjectDocument22 pagesCommunity Health Adpie Projectapi-461978440No ratings yet
- G PerinataloralhealthcareDocument6 pagesG PerinataloralhealthcareRosa WillisNo ratings yet
- Dental Pain and Associated Factors Among Pregnant Women: An Observational StudyDocument8 pagesDental Pain and Associated Factors Among Pregnant Women: An Observational StudyYafi HafizNo ratings yet
- Preventing Chronic DiseaseDocument9 pagesPreventing Chronic DiseaseBeatrice IancuNo ratings yet
- Oral Health and Menopause: A Comprehensive Review On Current Knowledge and Associated Dental ManagementDocument4 pagesOral Health and Menopause: A Comprehensive Review On Current Knowledge and Associated Dental ManagementFirman TirmaNo ratings yet
- Maternal ExposureDocument18 pagesMaternal ExposureFlórian JeffersonNo ratings yet
- Explain Why Some Mothers Lose Their Tooth/teeth Because of Multi-Pregnancy? Please Cite Some Concrete Evidences. (20 Points)Document2 pagesExplain Why Some Mothers Lose Their Tooth/teeth Because of Multi-Pregnancy? Please Cite Some Concrete Evidences. (20 Points)Luis Gatchalian LacanilaoNo ratings yet
- In Uence of Feeding Practices On Dental Caries. A Case-Control StudyDocument5 pagesIn Uence of Feeding Practices On Dental Caries. A Case-Control StudyNikmah's Dentist LifeNo ratings yet
- Knowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral Health - PMCDocument15 pagesKnowledge of Pregnant Women About Pregnancy Gingivitis and Children Oral Health - PMCoreosforthecaptainNo ratings yet
- Oral Health Pregnancy Res GuideDocument36 pagesOral Health Pregnancy Res GuidemargauxNo ratings yet
- Periodontal Status in Pregnant Women in Comparison With Non-Pregnant IndividualsDocument4 pagesPeriodontal Status in Pregnant Women in Comparison With Non-Pregnant IndividualsnurainiNo ratings yet
- Dentists' Knowledge of Oral Health During PregnancyDocument6 pagesDentists' Knowledge of Oral Health During PregnancyRubilu ResNo ratings yet
- Promoting Oral HealthDocument12 pagesPromoting Oral HealthJose Fernando Díez ConchaNo ratings yet
- Nutritional Status and Its Effect On Dental HealthDocument5 pagesNutritional Status and Its Effect On Dental HealthMemex papNo ratings yet
- Barriesr in Oral Health CareDocument2 pagesBarriesr in Oral Health CareRisana RahoofNo ratings yet
- Basic Oral Care For Patients With DysphagiaDocument9 pagesBasic Oral Care For Patients With DysphagiaAngélica GarcíaNo ratings yet
- Guideline On Perinatal Oral Health Care: Originating Council AdoptedDocument5 pagesGuideline On Perinatal Oral Health Care: Originating Council AdoptedFer Panda Vr RmNo ratings yet
- Oral Health 1-3&5Document38 pagesOral Health 1-3&5Umar FarouqNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Rizki Cah KeratonNo ratings yet
- La On Pregnant PatientsDocument5 pagesLa On Pregnant Patientsapi-702714333No ratings yet
- Ajnr 130Document16 pagesAjnr 130GRF PUBLISHERSNo ratings yet
- Dental Care Throughout Pregnancy: Do's and Don'tsDocument3 pagesDental Care Throughout Pregnancy: Do's and Don'tsdrzana78No ratings yet
- 7838 Periodontal Diseases and Adverse Pregnancy OutcomesDocument24 pages7838 Periodontal Diseases and Adverse Pregnancy OutcomesNgọc LinhNo ratings yet
- Benefits & Issues With Birth Control - Based On The Teachings Of Dr. Andrew Huberman: A Double-Edged Sword – Discovering The Positives And PitfallsFrom EverandBenefits & Issues With Birth Control - Based On The Teachings Of Dr. Andrew Huberman: A Double-Edged Sword – Discovering The Positives And PitfallsNo ratings yet
- Article - 1653239529 2Document5 pagesArticle - 1653239529 2Mega AzzahraNo ratings yet
- Internship JournalDocument3 pagesInternship Journalapi-491571677No ratings yet
- Research Article: International Journal of Current ResearchDocument4 pagesResearch Article: International Journal of Current ResearchSelvaNo ratings yet
- Pit and Fissure Sealants FinalDocument54 pagesPit and Fissure Sealants FinalAj VishwadheebNo ratings yet
- Autogenous Bone Is It Still The Gold Standard .1Document1 pageAutogenous Bone Is It Still The Gold Standard .1Andrea AriasNo ratings yet
- CamouflageDocument81 pagesCamouflageRohini TondaNo ratings yet
- Theories of GrowthDocument137 pagesTheories of GrowthYuvashreeNo ratings yet
- Anatomy of The Oral CavityDocument56 pagesAnatomy of The Oral CavitySaidu TanimuNo ratings yet
- Oral Lec 8Document9 pagesOral Lec 8Adam AliraqiNo ratings yet
- Treatment Options For The Compromised Tooth: A Decision GuideDocument16 pagesTreatment Options For The Compromised Tooth: A Decision GuidePuneet ChahalNo ratings yet
- An Insight in To Functionally Generated Pathway: A Review ArticleDocument7 pagesAn Insight in To Functionally Generated Pathway: A Review ArticlejancyNo ratings yet
- Vanlioglu. Retrospective Analysis of Prosthetic ComplicationsDocument5 pagesVanlioglu. Retrospective Analysis of Prosthetic ComplicationsNucleo AlgodonesNo ratings yet
- ACIIDA - SP - 1 Direct Anterior ApproachDocument30 pagesACIIDA - SP - 1 Direct Anterior ApproachJayjeet BhoiteNo ratings yet
- BPOC GuidelinesDocument15 pagesBPOC GuidelinesTeresa Perdon GarciaNo ratings yet
- 7 8 9 10 LecturesDocument17 pages7 8 9 10 LecturesYahya AbdNo ratings yet
- Preventive Dentistry 1Document19 pagesPreventive Dentistry 1blue nNo ratings yet
- The Altered Cast Impression Technique Revisited: Case ReportDocument6 pagesThe Altered Cast Impression Technique Revisited: Case ReportNiaz AhammedNo ratings yet
- DAC First Quarter 2021Document52 pagesDAC First Quarter 2021Armi CaberoNo ratings yet
- Russian For Everybody PDFDocument544 pagesRussian For Everybody PDFDilsonGomes88% (8)
- The Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North AmerDocument9 pagesThe Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North Amerlaljadeff12No ratings yet
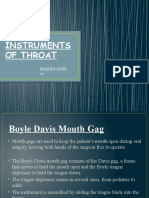
- Instruments of Throat: Sparsh Goel 77Document19 pagesInstruments of Throat: Sparsh Goel 77Sparsh GoelNo ratings yet
- Dhy 2020-21 Plan-Of-StudyDocument2 pagesDhy 2020-21 Plan-Of-Studyapi-546773895No ratings yet
- The TMJ - Admission ExamDocument22 pagesThe TMJ - Admission ExamAliaa NasserNo ratings yet
- Step4 - Multi UnitDocument28 pagesStep4 - Multi UnitSebastian MalagambaNo ratings yet
- DNH Pinning Program - 2021Document3 pagesDNH Pinning Program - 2021Christina QuirosNo ratings yet
- Reducing Dental Anxiety in Pediatric PatientsDocument6 pagesReducing Dental Anxiety in Pediatric Patientsapi-613602373No ratings yet
- An 2/2 Implant Overdenture: Case ReportDocument3 pagesAn 2/2 Implant Overdenture: Case ReportasclepiuspdfsNo ratings yet
- Shade Guides Used in The Dental PracticeDocument6 pagesShade Guides Used in The Dental PracticeNurul Khadijah HannbNo ratings yet
- Debate Acrylic Vs Cobalt ChromeDocument29 pagesDebate Acrylic Vs Cobalt ChromeNafij JamayetNo ratings yet
- EJMCM - Volume 7 - Issue 7 - Pages 381-390Document10 pagesEJMCM - Volume 7 - Issue 7 - Pages 381-390Hanina mamiNo ratings yet