You might also like
- 019 Foot and Ankle ClassificationsDocument13 pages019 Foot and Ankle ClassificationsOh Deh100% (1)
- Sexual Experiences of Women During Childbirth by Danielle HarelDocument141 pagesSexual Experiences of Women During Childbirth by Danielle HarelDelsa Vador100% (1)
- Statistical Process Monitoring Using Advanced Data-Driven and Deep Learning Approaches: Theory and Practical ApplicationsFrom EverandStatistical Process Monitoring Using Advanced Data-Driven and Deep Learning Approaches: Theory and Practical ApplicationsNo ratings yet
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 pagesDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- Electronic Prescribing Final ReportDocument92 pagesElectronic Prescribing Final ReportNuredin Abdumalik100% (1)
- Hospital Management SystemDocument51 pagesHospital Management SystemVishad Vats89% (9)
- Hemodynamic MonitoringDocument44 pagesHemodynamic Monitoringinvisigoth17No ratings yet
- Hospital Management SystemDocument29 pagesHospital Management SystemBWEB SOLUTIONSNo ratings yet
- Orthopaedics PunchDocument6 pagesOrthopaedics PunchHicham GawishNo ratings yet
- An Introduction to Healthcare Informatics: Building Data-Driven ToolsFrom EverandAn Introduction to Healthcare Informatics: Building Data-Driven ToolsRating: 5 out of 5 stars5/5 (1)
- HospitalDocument161 pagesHospitalAssad100% (1)
- Paediatrics Osce Cases (Hematology Dept)Document6 pagesPaediatrics Osce Cases (Hematology Dept)Nur Impiana100% (3)
- Re-Engineering Clinical Trials: Best Practices for Streamlining the Development ProcessFrom EverandRe-Engineering Clinical Trials: Best Practices for Streamlining the Development ProcessPeter SchuelerRating: 2 out of 5 stars2/5 (1)
- 09.Project-Hospital Management SystemDocument50 pages09.Project-Hospital Management SystemRajeev Ranjan89% (91)
- Pragmatic Randomized Clinical Trials: Using Primary Data Collection and Electronic Health RecordsFrom EverandPragmatic Randomized Clinical Trials: Using Primary Data Collection and Electronic Health RecordsCynthia J. GirmanNo ratings yet
- A Measurement Framework for Software Projects: A Generic and Practical Goal-Question-Metric(Gqm) Based Approach.From EverandA Measurement Framework for Software Projects: A Generic and Practical Goal-Question-Metric(Gqm) Based Approach.No ratings yet
- Hospital Management System For The Mayo Clinic - VFDocument26 pagesHospital Management System For The Mayo Clinic - VFGaurav94% (17)
- Design and Implementation of Appointment Management System (A CASE STUDY OF Federal Medical Center (FMC) .)Document52 pagesDesign and Implementation of Appointment Management System (A CASE STUDY OF Federal Medical Center (FMC) .)DAVIS ISIBOR100% (4)
- 2.emerging Technology in Nursing Practice PDFDocument89 pages2.emerging Technology in Nursing Practice PDFgao1989100% (2)
- A Manager's Guide to the Design and Conduct of Clinical TrialsFrom EverandA Manager's Guide to the Design and Conduct of Clinical TrialsNo ratings yet
- Hospital Management System - Prem AnandDocument14 pagesHospital Management System - Prem AnandPrem Anand100% (3)
- Statistical Monitoring of Complex Multivatiate Processes: With Applications in Industrial Process ControlFrom EverandStatistical Monitoring of Complex Multivatiate Processes: With Applications in Industrial Process ControlNo ratings yet
- Health Management Information System (HMIS)Document39 pagesHealth Management Information System (HMIS)Liza SethyNo ratings yet
- HipertiroidDocument31 pagesHipertiroidEdo Pramana PutraNo ratings yet
- Innovation in Clinical Trial Methodologies: Lessons Learned during the Corona PandemicFrom EverandInnovation in Clinical Trial Methodologies: Lessons Learned during the Corona PandemicPeter SchuelerRating: 3 out of 5 stars3/5 (1)
- Energy Efficiency of Medical Devices and Healthcare ApplicationsFrom EverandEnergy Efficiency of Medical Devices and Healthcare ApplicationsAmr MohamedNo ratings yet
- Measuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsFrom EverandMeasuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsNo ratings yet
- Big Data Analytics for Healthcare: Datasets, Techniques, Life Cycles, Management, and ApplicationsFrom EverandBig Data Analytics for Healthcare: Datasets, Techniques, Life Cycles, Management, and ApplicationsNo ratings yet
- Comm Service Report FormatDocument8 pagesComm Service Report FormatAmareNo ratings yet
- Lisa Gulker - 'The Chief Clinical Information Officer:Leading Innovation and Delivering Excellence'Document30 pagesLisa Gulker - 'The Chief Clinical Information Officer:Leading Innovation and Delivering Excellence'CCIONetworkNo ratings yet
- "Hospital Management System": Submited byDocument31 pages"Hospital Management System": Submited byNaveenNo ratings yet
- Hospital Patient Management SystemDocument53 pagesHospital Patient Management Systemmanthansingh0414No ratings yet
- Final SRS On Hospital Management SystemDocument24 pagesFinal SRS On Hospital Management SystemViranshi SanghaviNo ratings yet
- Shaping The Future of HealthcareDocument24 pagesShaping The Future of HealthcaresriramvsNo ratings yet
- Nurs 390 Group 8 Project 2Document31 pagesNurs 390 Group 8 Project 2api-621660715No ratings yet
- Hospital's Patient Records Managing Web Using PHP, MySqlDocument14 pagesHospital's Patient Records Managing Web Using PHP, MySqlSaurabh RajputNo ratings yet
- ProjectDocument88 pagesProjectManash KumarNo ratings yet
- 3nursing Informatics Class Notes 2020Document20 pages3nursing Informatics Class Notes 2020Ramya PamidimukkalaNo ratings yet
- Termpaepr - Hospital Management SystemsDocument20 pagesTermpaepr - Hospital Management SystemsSaif ShakilNo ratings yet
- Project Risk Final PaperDocument25 pagesProject Risk Final PaperSitota KebedeNo ratings yet
- Susan SEDocument33 pagesSusan SESusan GaireNo ratings yet
- Project PPT Shashank-1Document9 pagesProject PPT Shashank-1Shashank MoundekarNo ratings yet
- Documentation-Chapter 1 & 2Document16 pagesDocumentation-Chapter 1 & 2panget moNo ratings yet
- NCMB210 Final (11-17)Document14 pagesNCMB210 Final (11-17)Makspeyn del Valle - MoonNo ratings yet
- HCIN 545 Project 2 Group C: - Haripriya Munagala - Anu Mathew - Jo Tzu LiuDocument19 pagesHCIN 545 Project 2 Group C: - Haripriya Munagala - Anu Mathew - Jo Tzu LiuDoris LiuNo ratings yet
- Systems Design for Remote HealthcareFrom EverandSystems Design for Remote HealthcareKoushik MaharatnaNo ratings yet
- Developing Medical Apps and mHealth Interventions: A Guide for Researchers, Physicians and InformaticiansFrom EverandDeveloping Medical Apps and mHealth Interventions: A Guide for Researchers, Physicians and InformaticiansNo ratings yet
- Statistics for Censored Environmental Data Using Minitab and RFrom EverandStatistics for Censored Environmental Data Using Minitab and RNo ratings yet
- Information Technology in Pharmacy: An Integrated ApproachFrom EverandInformation Technology in Pharmacy: An Integrated ApproachNo ratings yet
- Implementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentFrom EverandImplementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentNo ratings yet
- Clinical Data Manager - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandClinical Data Manager - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Towards best practice in the Archetype Development ProcessFrom EverandTowards best practice in the Archetype Development ProcessNo ratings yet
- Comprehensive Care Coordination for Chronically Ill AdultsFrom EverandComprehensive Care Coordination for Chronically Ill AdultsCheryl SchraederNo ratings yet
- Pothole Terminator Can Be UsedDocument1 pagePothole Terminator Can Be UsedseeratNo ratings yet
- Sample File-1 PDFDocument1 pageSample File-1 PDFseeratNo ratings yet
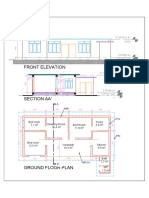
- Front Elevation: 3.1st Floor LVL 3350Document1 pageFront Elevation: 3.1st Floor LVL 3350seeratNo ratings yet
- Kolkata The City of Joy: MD Aquib Jawed byDocument55 pagesKolkata The City of Joy: MD Aquib Jawed byseeratNo ratings yet
- Walter GropiusDocument11 pagesWalter GropiusseeratNo ratings yet
- Questions. HIMYMDocument1 pageQuestions. HIMYMseeratNo ratings yet
- Artist'S House: (Autocad)Document1 pageArtist'S House: (Autocad)seeratNo ratings yet
- Quick Guide To Prescribing, Medicine Supplies and Support From Your PharmacyDocument11 pagesQuick Guide To Prescribing, Medicine Supplies and Support From Your Pharmacyminhmap90_635122804No ratings yet
- We Want The Airwaves - Star Amerasu PT 1Document9 pagesWe Want The Airwaves - Star Amerasu PT 1Nia KingNo ratings yet
- BrachytherapyDocument10 pagesBrachytherapyapi-279886264No ratings yet
- Nursing PhilosophyDocument5 pagesNursing Philosophyapi-532524779No ratings yet
- Maternal Collapse in Pregnancy and The Puerperium: Green-Top Guideline No. 56Document39 pagesMaternal Collapse in Pregnancy and The Puerperium: Green-Top Guideline No. 56wai lynnNo ratings yet
- PositioningDocument26 pagesPositioningsunielgowda100% (1)
- Interventions of Postpartum Hemorrhage.16Document17 pagesInterventions of Postpartum Hemorrhage.16Fernando Peralta PalmezanoNo ratings yet
- Pan Am Rehab Symposium 2019 Lumbar SpineDocument2 pagesPan Am Rehab Symposium 2019 Lumbar SpineGusti TettaNo ratings yet
- Comparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GDocument14 pagesComparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GIJAR JOURNALNo ratings yet
- ACCREDITATIONDocument62 pagesACCREDITATIONMargeYagoJulianoNo ratings yet
- CGHS Empanelled Hospitals May2019Document18 pagesCGHS Empanelled Hospitals May2019ganesan19754573No ratings yet
- Expanded Disability Status Scale (EDSS) : Scor e DescriptionDocument2 pagesExpanded Disability Status Scale (EDSS) : Scor e DescriptionChe AinNo ratings yet
- Ipmr AbbreviationsDocument2 pagesIpmr Abbreviationsapi-258242054No ratings yet
- HISTOLOGY of Organs Associated With The Digestive Tract For 2nd Year Mbbs (By DR Sundus)Document25 pagesHISTOLOGY of Organs Associated With The Digestive Tract For 2nd Year Mbbs (By DR Sundus)Mudassar RoomiNo ratings yet
- Antenatal Fitness Sessions Poster May21Document3 pagesAntenatal Fitness Sessions Poster May21Sameer UddinNo ratings yet
- Windshield SurveyDocument20 pagesWindshield Surveyapi-260551351No ratings yet
- Icd 10 Code Klinik DR KeluargaDocument6 pagesIcd 10 Code Klinik DR Keluargaferry7765No ratings yet
- Daftar Pustaka Per BabDocument4 pagesDaftar Pustaka Per BabMuhammad Harry Badrus SNo ratings yet
- Pregnant Women Invitation LetterDocument3 pagesPregnant Women Invitation LetterDulanjalee SachittraNo ratings yet
- PartographDocument1 pagePartographVraj SoniNo ratings yet
- C/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromDocument5 pagesC/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromarsohgahNo ratings yet
- MukokelDocument3 pagesMukokeljulietNo ratings yet
- Dr. Hur JunDocument2 pagesDr. Hur JunMegha GoyalNo ratings yet