You might also like
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Pharmacologic Agents in Heart Failure: Ayman Khdair, Ph.D. Wayne State University, Michigan, USADocument41 pagesPharmacologic Agents in Heart Failure: Ayman Khdair, Ph.D. Wayne State University, Michigan, USAJalil HaddadinNo ratings yet
- СердечнаяDocument70 pagesСердечнаяDaniel FunkNo ratings yet
- Drugs Used in The Management of Heart Failure: DR Sindwa KanyimbaDocument29 pagesDrugs Used in The Management of Heart Failure: DR Sindwa Kanyimbaedward kaumbaNo ratings yet
- Manage Cardiac EmergenciesDocument56 pagesManage Cardiac Emergencies21rayhanf100% (1)
- Erasmus Heart DrugsDocument90 pagesErasmus Heart DrugsDanilo ČešljaracNo ratings yet
- Drugs Acting in CVSDocument63 pagesDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- 2022 Pharmacology s2t2 HeartfailureDocument6 pages2022 Pharmacology s2t2 Heartfailurejed larsen capulong gavinoNo ratings yet
- 7MB, Ac, 1PCSDocument1 page7MB, Ac, 1PCSRicko CiadyNo ratings yet
- Unit 2 Heart Failure: StructureDocument29 pagesUnit 2 Heart Failure: StructurebtaleraNo ratings yet
- ShockDocument16 pagesShockChristiaan VoslooNo ratings yet
- Cardiac PharmDocument6 pagesCardiac PharmJohn SmithNo ratings yet
- LOW Cardiac Output: Use of Inotropes in Critical CareDocument5 pagesLOW Cardiac Output: Use of Inotropes in Critical CareRiimsha AaymNo ratings yet
- Drugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3Document47 pagesDrugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3DR Muhammad Abdul BasitNo ratings yet
- Congestive Heart Failure PDFDocument11 pagesCongestive Heart Failure PDFpriyanka bhavsarNo ratings yet
- Cardiovascular Agents Group 1 Parmacology ReportingDocument415 pagesCardiovascular Agents Group 1 Parmacology ReportingMajestic RavenNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Heart Failure: Causes, Treatments, and Dental ImplicationsDocument8 pagesHeart Failure: Causes, Treatments, and Dental Implicationsمحمد علي حميدNo ratings yet
- Chronic Heart Failure: I. Brief Definition Iv. Disease ProcessDocument12 pagesChronic Heart Failure: I. Brief Definition Iv. Disease ProcessJennifer BeguinwaNo ratings yet
- Treating Congestive Heart Failure with Diuretics, Inotropes, Vasodilators and ACE InhibitorsDocument18 pagesTreating Congestive Heart Failure with Diuretics, Inotropes, Vasodilators and ACE InhibitorsAnityo NugrohoNo ratings yet
- Cardiogenic Shock Causes and TreatmentDocument43 pagesCardiogenic Shock Causes and TreatmentGalih Arief Harimurti WawolumajaNo ratings yet
- Heart Failure - 2022Document106 pagesHeart Failure - 2022Rana Khaled AwwadNo ratings yet
- Problem Based Learning Cardiovascular System: 2nd GroupDocument47 pagesProblem Based Learning Cardiovascular System: 2nd GroupClaudia Narinda R. PNo ratings yet
- Heart Failure New SlidesDocument41 pagesHeart Failure New SlidesjawadNo ratings yet
- Acute Heart FailureDocument18 pagesAcute Heart FailureGeorge GeorgeNo ratings yet
- Diagnosis&Manajemen ShockDocument8 pagesDiagnosis&Manajemen ShockHJKIMNo ratings yet
- Asist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and ToxicologyDocument52 pagesAsist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and Toxicologyمصطفى ابراهيم سعيدNo ratings yet
- Drugs Used in Heart Failure: Pharmacology (2) PHAR 342Document19 pagesDrugs Used in Heart Failure: Pharmacology (2) PHAR 342Dana HamarshehNo ratings yet
- MedicationsDocument30 pagesMedicationsvamshidhNo ratings yet
- Heart FailureDocument14 pagesHeart Failurelandita683No ratings yet
- Cardiovascular Drugs (Veterinary Pharmacology)Document44 pagesCardiovascular Drugs (Veterinary Pharmacology)DR Muhammad Abdul BasitNo ratings yet
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNo ratings yet
- Cardiogenic ShockDocument29 pagesCardiogenic ShockagnescheruseryNo ratings yet
- Heart FailureDocument44 pagesHeart FailureSalman Habeeb100% (6)
- Patofisiologi Shock CardiogenicDocument44 pagesPatofisiologi Shock CardiogenicGalih Arief Harimurti Wawolumaja100% (1)
- Drugs For CHF & Angina PDFDocument15 pagesDrugs For CHF & Angina PDFAbdullah ElsayedNo ratings yet
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- Heart Failur E: Nitish Kumar Maddhesia, 74Document26 pagesHeart Failur E: Nitish Kumar Maddhesia, 74Akash NagarNo ratings yet
- ADHF Wecoc FinalDocument27 pagesADHF Wecoc FinalNovrian Ali YlberNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Manage Cardiac Medications EffectivelyDocument2 pagesManage Cardiac Medications EffectivelyVincent Paul SantosNo ratings yet
- NCP Partial, Micu Medcor DutyDocument7 pagesNCP Partial, Micu Medcor DutyYana PotNo ratings yet
- Cardiogenic ShockDocument20 pagesCardiogenic Shockanimesh pandaNo ratings yet
- Nursing Care Plan for HypotensionDocument2 pagesNursing Care Plan for HypotensiondubsNo ratings yet
- Vasoactive Drugs GuideDocument14 pagesVasoactive Drugs GuideTushar GhuleNo ratings yet
- Drug Study: ER DrugsDocument5 pagesDrug Study: ER Drugsmaeca101No ratings yet
- Nursing Care Plan for HypotensionDocument2 pagesNursing Care Plan for HypotensionMae Denn LabordoNo ratings yet
- Cardiogenic Shock Causes and TreatmentDocument5 pagesCardiogenic Shock Causes and Treatmental-obinay shereenNo ratings yet
- CVS DiseasesDocument15 pagesCVS DiseasesNaavaNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Risk For Decreased Cardiac Output: Nursing DiagnosisDocument4 pagesRisk For Decreased Cardiac Output: Nursing DiagnosisRiska RamadaniNo ratings yet
- CHF LastDocument52 pagesCHF LastAli YousefNo ratings yet
- P 3a Gagal JTGDocument35 pagesP 3a Gagal JTGAnaMariyaMaNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- Drugs Used in The Treatment of Congestive Heart FailureDocument18 pagesDrugs Used in The Treatment of Congestive Heart Failurekarina azlia amandaNo ratings yet
- Cardiovascular DiseaseDocument14 pagesCardiovascular DiseasenonameNo ratings yet
- An Unusual, Reversible Cause of Acute High-Outpout HFDocument5 pagesAn Unusual, Reversible Cause of Acute High-Outpout HFPeter Albeiro Falla CortesNo ratings yet
- Lec 3 Heart FailureDocument25 pagesLec 3 Heart FailureDelete AccountNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Developmental MilestonesDocument18 pagesDevelopmental MilestonesCarly Beth Caparida LangerasNo ratings yet
- Analytical Phase ResearchDocument5 pagesAnalytical Phase ResearchCarly Beth Caparida LangerasNo ratings yet
- Analytical Phase ResearchDocument5 pagesAnalytical Phase ResearchCarly Beth Caparida LangerasNo ratings yet
- Developmental MilestonesDocument18 pagesDevelopmental MilestonesCarly Beth Caparida LangerasNo ratings yet
- Pathophysiology of Hypertension, Diabetes, Ubm, BPHDocument3 pagesPathophysiology of Hypertension, Diabetes, Ubm, BPHCarly Beth Caparida LangerasNo ratings yet
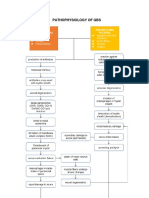
- Pathophysiology of GbsDocument3 pagesPathophysiology of GbsCarly Beth Caparida LangerasNo ratings yet
- Assessing Priority Systems for Bladder, Prostate, HTN & DiabetesDocument5 pagesAssessing Priority Systems for Bladder, Prostate, HTN & DiabetesCarly Beth Caparida LangerasNo ratings yet
- GBS Pathophysiology: Causes and MechanismsDocument3 pagesGBS Pathophysiology: Causes and MechanismsCarly Beth Caparida Langeras100% (1)
- CASE ANALYSIS (Diabetes)Document21 pagesCASE ANALYSIS (Diabetes)Carly Beth Caparida LangerasNo ratings yet
- CASE ANALYSIS (Diabetes)Document21 pagesCASE ANALYSIS (Diabetes)Carly Beth Caparida LangerasNo ratings yet
- Assessing Priority Systems for Bladder, Prostate, HTN & DiabetesDocument5 pagesAssessing Priority Systems for Bladder, Prostate, HTN & DiabetesCarly Beth Caparida LangerasNo ratings yet
- Case Study of Atherosclerosis 1. Risk Factors of AtherosclerosisDocument5 pagesCase Study of Atherosclerosis 1. Risk Factors of AtherosclerosisCarly Beth Caparida LangerasNo ratings yet
- Ibs (Conceptmap)Document4 pagesIbs (Conceptmap)Carly Beth Caparida LangerasNo ratings yet
- Child Immunization SchedulerDocument2 pagesChild Immunization SchedulerxtineNo ratings yet
- Dental Considerations of Patient With Liver DiseaseDocument14 pagesDental Considerations of Patient With Liver DiseaseManas MksNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsSanchita KunwerNo ratings yet
- Jiggar DrugsDocument3 pagesJiggar DrugsRockeven DesirNo ratings yet
- Template Article UpdateDocument11 pagesTemplate Article UpdateAnggun SasmitaNo ratings yet
- Presentasi Radiologi Edema ParuDocument19 pagesPresentasi Radiologi Edema ParuFia100% (1)
- Nursing Care Plan for HyperthermiaDocument2 pagesNursing Care Plan for HyperthermiaJhensczy Hazel Maye AlbaNo ratings yet
- ITOM Group Assignment Issues at SCHDocument12 pagesITOM Group Assignment Issues at SCHzeeraNo ratings yet
- AIIMS Protocol On Shock 2019Document16 pagesAIIMS Protocol On Shock 2019gaddam narasimhaNo ratings yet
- Paramedic Inter Facility Transfer TrainingDocument168 pagesParamedic Inter Facility Transfer TrainingnikunjhirparaNo ratings yet
- Inguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsDocument24 pagesInguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsmutmainnahNo ratings yet
- 10 Classifications of Drugs and Their Effects ExplainedDocument4 pages10 Classifications of Drugs and Their Effects ExplainedAirish GeronimoNo ratings yet
- Opportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaDocument4 pagesOpportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaPinay YaunNo ratings yet
- EBM TerapiDocument23 pagesEBM TerapidyahayulestariNo ratings yet
- Report On COVID-19 Outbreak at Holyoke Soldiers' HomeDocument174 pagesReport On COVID-19 Outbreak at Holyoke Soldiers' HomeGreg Saulmon100% (8)
- Femto-Lasik laser eye surgery explainedDocument4 pagesFemto-Lasik laser eye surgery explainedvrlftrNo ratings yet
- WNHS OG PregnancyFirstTrimesterDocument60 pagesWNHS OG PregnancyFirstTrimesterBharata YudhaNo ratings yet
- Open - Oregonstate.education-Foundations of EpidemiologyDocument11 pagesOpen - Oregonstate.education-Foundations of EpidemiologyAMANE COTTAGE HOSPITALNo ratings yet
- Bakson ApplDocument1 pageBakson ApplSwayam Prava DasNo ratings yet
- SP Care Health Promo Oct-Nov 2021Document3 pagesSP Care Health Promo Oct-Nov 2021Dr Uvarani Sp Care Rawang TinNo ratings yet
- Helicure - Google SearchDocument1 pageHelicure - Google Searchalijan deparNo ratings yet
- Family Dynamics and Assessment Tools: Dr. Oryzati Hilman Agrimon, MSC - CMFM, PHD (C)Document40 pagesFamily Dynamics and Assessment Tools: Dr. Oryzati Hilman Agrimon, MSC - CMFM, PHD (C)Ther Ray100% (1)
- Stree Roga Vigyan-Mallikarjuna With MCQs PDFDocument20 pagesStree Roga Vigyan-Mallikarjuna With MCQs PDFCHAUKHAMBHA PRAKASHAKNo ratings yet
- Cash, Receivables, Inventory, and Asset AccountsDocument19 pagesCash, Receivables, Inventory, and Asset Accountsvina tNo ratings yet
- ODB Funda of Pharma NLEDocument4 pagesODB Funda of Pharma NLEMarisol DizonNo ratings yet
- Dengue Discharge PlanDocument6 pagesDengue Discharge PlanChayliu Bugo75% (4)
- Steps in Outbreak InvestigationDocument34 pagesSteps in Outbreak Investigationsharmaine peroNo ratings yet
- AIDS Link To Smallpox VaccineDocument3 pagesAIDS Link To Smallpox Vaccinehenrikas3970No ratings yet
- Anthony J. Destefano, PHD: Growing ThreatsDocument23 pagesAnthony J. Destefano, PHD: Growing Threatstamuno7No ratings yet
- Monitoring Vital Signs Detects COVID-19 Using WearablesDocument7 pagesMonitoring Vital Signs Detects COVID-19 Using WearablesMaxandrea Beatrice ArmillaNo ratings yet