You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Human and Social Biology SBADocument12 pagesHuman and Social Biology SBATamoy Noble100% (1)
- Pre-Intermediate, Chapter 1 Test: Select Readings, Second EditionDocument2 pagesPre-Intermediate, Chapter 1 Test: Select Readings, Second Editionreihaneh azimi100% (1)
- Capillary Blood Glucose (CBG) Examination Study Guide: NCM - 116 - Related Learning Experience (Skills and ClinicalDocument15 pagesCapillary Blood Glucose (CBG) Examination Study Guide: NCM - 116 - Related Learning Experience (Skills and ClinicalAlma Janella TOSINONo ratings yet
- Vertigo For GP - How To Approach It - Dr. Ni Nengah Rida AriariniDocument21 pagesVertigo For GP - How To Approach It - Dr. Ni Nengah Rida AriariniAsiatiNo ratings yet
- Dr. Waluyo Rudiyanto, M.KesDocument50 pagesDr. Waluyo Rudiyanto, M.KesAsiatiNo ratings yet
- Furo Menu A4 Compressed 2 1Document17 pagesFuro Menu A4 Compressed 2 1AsiatiNo ratings yet
- Update On Systemic Glucocorticosteroids in Dermatology: C. MD, T. MDDocument15 pagesUpdate On Systemic Glucocorticosteroids in Dermatology: C. MD, T. MDAsiatiNo ratings yet
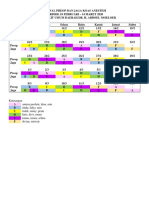
- JADWAL KOAS ANESTESI 10 Feb - 14 MarDocument2 pagesJADWAL KOAS ANESTESI 10 Feb - 14 MarAsiatiNo ratings yet
- Alamanda'S 2 Floor: Rifqi Fadhil M Helen Kusuma WDocument4 pagesAlamanda'S 2 Floor: Rifqi Fadhil M Helen Kusuma WAsiatiNo ratings yet
- Skin To SkinDocument9 pagesSkin To SkinAsiatiNo ratings yet
- DO - Public Speaking (Dr. Dwita Oktaria, M.PD - Ked.)Document42 pagesDO - Public Speaking (Dr. Dwita Oktaria, M.PD - Ked.)AsiatiNo ratings yet
- 23 Agt InggrisDocument17 pages23 Agt InggrisAsiatiNo ratings yet
- 1 PB PDFDocument10 pages1 PB PDFAsiatiNo ratings yet
- CV MR Dec19Document6 pagesCV MR Dec19AsiatiNo ratings yet
- The Relationship Between The Big Five Personality Factors With Blood Types inDocument8 pagesThe Relationship Between The Big Five Personality Factors With Blood Types inAsiatiNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document7 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Mach BoosDocument2 pagesMach Boosmutawa510No ratings yet
- Diabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDDocument23 pagesDiabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيار100% (1)
- Diabetes FlowchartDocument1 pageDiabetes Flowcharthhos619No ratings yet
- The Use of Cgms in Redefining Care Delivery For Type 2 DiabetesDocument8 pagesThe Use of Cgms in Redefining Care Delivery For Type 2 DiabetesChrisSandersNo ratings yet
- Children Presentation Nutrition and DiabetesDocument19 pagesChildren Presentation Nutrition and Diabetesapi-516120803No ratings yet
- Poverty Increases Type 2 Diabetes Incidence and Inequality of Care Despite Universal Health CoverageDocument7 pagesPoverty Increases Type 2 Diabetes Incidence and Inequality of Care Despite Universal Health CoverageHitmanNo ratings yet
- Schmitt Et Al jpr2017 Depression-Related HyperglycaemiaDocument7 pagesSchmitt Et Al jpr2017 Depression-Related HyperglycaemiaTiToNo ratings yet
- ASHITABA Vs Gynura ProcumbensDocument6 pagesASHITABA Vs Gynura ProcumbensRica Santos100% (1)
- Marketing Management (MKT201) : Term Individual Assignment On Assignment - 3Document6 pagesMarketing Management (MKT201) : Term Individual Assignment On Assignment - 3VIPUL TUTEJANo ratings yet
- Insulin in Pregnancy: Dr. Kyar Nyo Soe Myint Consultant Endocrinologist University of Medicine 2, NOGTHDocument39 pagesInsulin in Pregnancy: Dr. Kyar Nyo Soe Myint Consultant Endocrinologist University of Medicine 2, NOGTHYadanar KyawNo ratings yet
- DiabeticwhitepapernamesDocument77 pagesDiabeticwhitepapernamesManishNo ratings yet
- Hypoglycemia in NewbornDocument10 pagesHypoglycemia in Newbornmaxim tomuNo ratings yet
- Glycemic Management in The Operating RoomDocument13 pagesGlycemic Management in The Operating Room凌晓敏No ratings yet
- Ada Soc Diabetes in Hospital SettingDocument10 pagesAda Soc Diabetes in Hospital SettingOchie YecyecanNo ratings yet
- contentPDFs 2023 T2DM Pharmacotherapy Chart V2-2Document2 pagescontentPDFs 2023 T2DM Pharmacotherapy Chart V2-2El MaheritoNo ratings yet
- HypertensionDocument2 pagesHypertensionheadseNo ratings yet
- Incentive Calculation HWC-SC: 2021-2022 3 February No. of AshasDocument2 pagesIncentive Calculation HWC-SC: 2021-2022 3 February No. of AshasShreeya ShahNo ratings yet
- DNP Project FinalDocument40 pagesDNP Project Finalapi-521620733No ratings yet
- Irene's Care StudyDocument68 pagesIrene's Care StudyLawrence AckahNo ratings yet
- dmt2 LansiaDocument3 pagesdmt2 LansiaLavenia Juliani100% (1)
- CreatinineDocument3 pagesCreatinineElixirNo ratings yet
- Bayer Breeze2 User ManualDocument55 pagesBayer Breeze2 User ManualYvan Jacen ErnacioNo ratings yet
- Amanda Shelvia Savitri - The Genetic Factors of T2DDocument7 pagesAmanda Shelvia Savitri - The Genetic Factors of T2DAmanda Shelvia SavitriNo ratings yet
- Dapus AbrorDocument2 pagesDapus AbrorZulfitrawatiNo ratings yet
- Consulta FarmacoterapéuticaDocument13 pagesConsulta FarmacoterapéuticaNano NoratoNo ratings yet
- Management of Diabetes Emergencies''Document85 pagesManagement of Diabetes Emergencies''Princewill SeiyefaNo ratings yet