You might also like
- Graftless Solutions for the Edentulous PatientFrom EverandGraftless Solutions for the Edentulous PatientSaj JivrajNo ratings yet
- Artéria PalatinaDocument9 pagesArtéria PalatinaJefferson ThomazNo ratings yet
- Tavellietal. 2018 WhatIstheSafetyZoneforPalatalSoftTissueGrDocument9 pagesTavellietal. 2018 WhatIstheSafetyZoneforPalatalSoftTissueGrKyoko CPNo ratings yet
- Greater Palatine ArteryDocument9 pagesGreater Palatine ArterySuli M ENo ratings yet
- Tavellietal. 2018 WhatIstheSafetyZoneforPalatalSoftTissueGrDocument10 pagesTavellietal. 2018 WhatIstheSafetyZoneforPalatalSoftTissueGrLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Articulo David RicucciDocument36 pagesArticulo David RicucciDaniela Cortes HernandezNo ratings yet
- Skeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsDocument6 pagesSkeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsRolando Huaman BravoNo ratings yet
- Efficacy o TunnelDocument42 pagesEfficacy o TunnelMacaa AriasNo ratings yet
- Jced 13 E75Document6 pagesJced 13 E75Ezza RezzaNo ratings yet
- The Buffalo Study Outcome and Associated Predictors in Endodontic Microsurgery A Cohort StudyDocument34 pagesThe Buffalo Study Outcome and Associated Predictors in Endodontic Microsurgery A Cohort StudyGinna Estefania TutasigNo ratings yet
- American Academy of Periodontology Best Evidence Consensus Statement On Modifying Peridontal Phenotype in Preparation For Orthodontic and Restorative Treatment 2019Document10 pagesAmerican Academy of Periodontology Best Evidence Consensus Statement On Modifying Peridontal Phenotype in Preparation For Orthodontic and Restorative Treatment 2019Implant DentNo ratings yet
- Outcome of Autotransplantation of Mature Third Molars Using 3-Dimensional-Printed Guiding Templates and Donor Tooth Replicas - 10. Estereo Aut 2019Document8 pagesOutcome of Autotransplantation of Mature Third Molars Using 3-Dimensional-Printed Guiding Templates and Donor Tooth Replicas - 10. Estereo Aut 2019Comisaría AsunciónNo ratings yet
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocument12 pagesBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNo ratings yet
- T-Cap 10091Document9 pagesT-Cap 10091Joshua Diaz QuiquijanaNo ratings yet
- Clinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyDocument10 pagesClinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyCamilo Andrés Sabogal ArguelloNo ratings yet
- Long Term Effects of Lateral Nasal Wall Anchored FDocument9 pagesLong Term Effects of Lateral Nasal Wall Anchored FRenan VeigaNo ratings yet
- Flap Approaches in Plastic Periodontal and Implant Surgery: Critical Elements in Design and ExecutionDocument15 pagesFlap Approaches in Plastic Periodontal and Implant Surgery: Critical Elements in Design and Executionxiaoxin zhangNo ratings yet
- Surgical Reconstruction of Interdental PDocument11 pagesSurgical Reconstruction of Interdental PMaria Jose GodoyNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Rara SumangandoNo ratings yet
- Clin Oral Invest BTCP Type 1 Col ConesDocument10 pagesClin Oral Invest BTCP Type 1 Col ConesPathivada LumbiniNo ratings yet
- Gingival Phenotype and Its Relationship With Different Clinical Parameters: A Study in A Dominican Adult SampleDocument7 pagesGingival Phenotype and Its Relationship With Different Clinical Parameters: A Study in A Dominican Adult SampleHarish ShahNo ratings yet
- CBCT Article DiagnosticsDocument17 pagesCBCT Article DiagnosticsNajla Dar-OdehNo ratings yet
- Ferrari Et Al 2017 JDentDocument29 pagesFerrari Et Al 2017 JDentAli Al-QaysiNo ratings yet
- Third Molar Autotransplant Planning With A Tooth Replica. A Year of Follow-Up Case ReportDocument6 pagesThird Molar Autotransplant Planning With A Tooth Replica. A Year of Follow-Up Case ReportAlNo ratings yet
- Dento Alveolar Measurements and Histomorphometric Parameters of Maxillary and Mandibular First Molars, Using Micro CTDocument12 pagesDento Alveolar Measurements and Histomorphometric Parameters of Maxillary and Mandibular First Molars, Using Micro CTBagis Emre GulNo ratings yet
- Evaluation of Mandibular Lingual Foramina Related To Dental Implant Treatment With Computerized Tomography: A Multicenter Clinical StudyDocument8 pagesEvaluation of Mandibular Lingual Foramina Related To Dental Implant Treatment With Computerized Tomography: A Multicenter Clinical Studyanimeilove3No ratings yet
- Nobre 2016Document10 pagesNobre 2016MonicaNo ratings yet
- Efecto de Las Preparaciones Dentales HorizontalesDocument7 pagesEfecto de Las Preparaciones Dentales HorizontalesJorge LucasNo ratings yet
- Dimensional Changes in Free Epithelialized Gingival/mucosal Grafts at Tooth and Implant Sites: A Prospective Cohort StudyDocument10 pagesDimensional Changes in Free Epithelialized Gingival/mucosal Grafts at Tooth and Implant Sites: A Prospective Cohort StudyDiana Pellecer de SmithNo ratings yet
- An Evaluation of Gingival Phenotype and Thickness As Determined by Indirect and Direct MethodsDocument8 pagesAn Evaluation of Gingival Phenotype and Thickness As Determined by Indirect and Direct MethodsAlfred OrozcoNo ratings yet
- Clin Implant Dent Rel Res - 2022 - Liu - Suggested Mesiodistal Distance For Multiple Implant Placement Based On The NaturalDocument8 pagesClin Implant Dent Rel Res - 2022 - Liu - Suggested Mesiodistal Distance For Multiple Implant Placement Based On The NaturalabarrientostorresNo ratings yet
- 1 R Cambios OSEOS POSEXTRACCIONDocument16 pages1 R Cambios OSEOS POSEXTRACCIONfeli.riam24No ratings yet
- Riesgo de Problema Periodontal Por OrtodonciaDocument18 pagesRiesgo de Problema Periodontal Por OrtodonciaenzoNo ratings yet
- Analysis of The Gingival Biotype Based On The Measurement of The Dentopapillary ComplexDocument6 pagesAnalysis of The Gingival Biotype Based On The Measurement of The Dentopapillary ComplexAngela ArrazolaNo ratings yet
- J Clinic Periodontology - 2015 - Yilmaz - Cone Beam Computed Tomography Evaluation of The Soft Tissue Thickness and GreaterDocument4 pagesJ Clinic Periodontology - 2015 - Yilmaz - Cone Beam Computed Tomography Evaluation of The Soft Tissue Thickness and GreaterjhynasindyNo ratings yet
- Sedacion Oral Dental OfficeDocument22 pagesSedacion Oral Dental OfficeAngélica Valenzuela AndrighiNo ratings yet
- Jper.19 0310 1Document13 pagesJper.19 0310 1Iga OktawisdoNo ratings yet
- JCM 09 00576Document9 pagesJCM 09 00576GABRIELA MOLANO MEZANo ratings yet
- Eruption AnomalyDocument7 pagesEruption AnomalyJay BernalNo ratings yet
- Implantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesDocument8 pagesImplantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesBagis Emre GulNo ratings yet
- Association of Gingival Biotype With The Results of Scaling and Root PlaningDocument8 pagesAssociation of Gingival Biotype With The Results of Scaling and Root PlaningYani YoelianiNo ratings yet
- DentogingivalComplex - Dimension Based On BiotypesDocument5 pagesDentogingivalComplex - Dimension Based On BiotypesAngela ArrazolaNo ratings yet
- Split Technique 3Document13 pagesSplit Technique 3Alejandro RuizNo ratings yet
- Assessment of Bone Dimensions in The Anterior Maxilla: A Cone Beam Computed Tomography StudyDocument8 pagesAssessment of Bone Dimensions in The Anterior Maxilla: A Cone Beam Computed Tomography Studylive your storyNo ratings yet
- 软组织相关的并发症风险Document15 pages软组织相关的并发症风险xiaoxin zhangNo ratings yet
- Practice-Based Clinical Evaluation of Zirconia PDFDocument12 pagesPractice-Based Clinical Evaluation of Zirconia PDFDiego Alejandro Cortés LinaresNo ratings yet
- 2019 Autogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical ReconstructionDocument8 pages2019 Autogenous Soft Tissue Grafting For Periodontal and Peri-Implant Plastic Surgical Reconstructionayu calisthaNo ratings yet
- 2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportDocument13 pages2020 - Stereolithographic Surgical Guide With A Combination of Tooth and Bone SupportVõHoàngThủyTiênNo ratings yet
- Retrieve 4Document8 pagesRetrieve 4dreneanastriNo ratings yet
- Journal of Periodontology - 2019 - Lin - The Significance of Surgically Modifying Soft Tissue Phenotype Around Fixed DentalDocument13 pagesJournal of Periodontology - 2019 - Lin - The Significance of Surgically Modifying Soft Tissue Phenotype Around Fixed DentalnassilaNo ratings yet
- Tipos de GuiasDocument8 pagesTipos de GuiasDr.CdiazNo ratings yet
- Factors Related To Microimplant Assisted Rapid PalDocument8 pagesFactors Related To Microimplant Assisted Rapid PalFernando Espada SalgadoNo ratings yet
- Journal ProstoDocument6 pagesJournal ProstoAvila Aita Harun RasyidNo ratings yet
- Influence of Diameter and Length of Implant On Early Dental Implant FailureDocument6 pagesInfluence of Diameter and Length of Implant On Early Dental Implant FailureCatalina AndreeaNo ratings yet
- Survival of Restored Endodontically Treated Teeth in Relation To Periodontal StatusDocument4 pagesSurvival of Restored Endodontically Treated Teeth in Relation To Periodontal StatusJing XueNo ratings yet
- Roll Man 2013Document6 pagesRoll Man 2013SergioNo ratings yet
- Vonarx 2012Document10 pagesVonarx 2012Laura A. Moraes PintoNo ratings yet
- Gon Alves 2014Document6 pagesGon Alves 2014saulNo ratings yet
- Meza-Mauricio 2021. b-3-6Document12 pagesMeza-Mauricio 2021. b-3-6MARIA ANTONIETA RODRIGUEZ GALECIONo ratings yet
- Ir 2016Document6 pagesIr 2016Banica alexandra carinaNo ratings yet
- Gingival Biotype Classification, Assessment, and Clinical Importance: A ReviewDocument7 pagesGingival Biotype Classification, Assessment, and Clinical Importance: A ReviewKetherin LeeNo ratings yet
- Assessment of Effect of Periodontal Biotype On Gingival Esthetics - A Study in North Gujarat PopulationDocument10 pagesAssessment of Effect of Periodontal Biotype On Gingival Esthetics - A Study in North Gujarat PopulationKetherin LeeNo ratings yet
- Akt OsteoDocument8 pagesAkt OsteoKetherin LeeNo ratings yet
- Cortellini Et Al-2018-Journal of Clinical PeriodontologyDocument9 pagesCortellini Et Al-2018-Journal of Clinical PeriodontologyErnestoNo ratings yet
- Mucogingival Conditions in The Natural DentitionDocument10 pagesMucogingival Conditions in The Natural DentitionMartty BaNo ratings yet
- Application Checklist: Background InformationDocument10 pagesApplication Checklist: Background InformationKetherin LeeNo ratings yet
- Harvard Business School Application ProcessDocument9 pagesHarvard Business School Application ProcessKetherin LeeNo ratings yet
- Microwave SterilizationDocument10 pagesMicrowave SterilizationKetherin LeeNo ratings yet
- Space Maintainers in Dentistry: Past To Present: Abst TDocument4 pagesSpace Maintainers in Dentistry: Past To Present: Abst TKetherin LeeNo ratings yet
- Treatment of Perforation of The Pulp CavityDocument10 pagesTreatment of Perforation of The Pulp CavityKetherin LeeNo ratings yet
- Efficacy of Hyaluronic Acid PDFDocument3 pagesEfficacy of Hyaluronic Acid PDFKetherin LeeNo ratings yet
- Treatment AlternativesDocument24 pagesTreatment AlternativesKetherin LeeNo ratings yet
- Kasus1 PDFDocument10 pagesKasus1 PDFKetherin LeeNo ratings yet
- Etiopathogenesis of Recurrent Aphthous Stomatitis and The Role of Immunologic Aspects: Literature ReviewDocument11 pagesEtiopathogenesis of Recurrent Aphthous Stomatitis and The Role of Immunologic Aspects: Literature ReviewAinun RamadaniNo ratings yet
- Journal Reading 1Document5 pagesJournal Reading 1Ketherin LeeNo ratings yet
- SRC InterviewDocument5 pagesSRC InterviewKetherin LeeNo ratings yet
- Journal Reading 1Document5 pagesJournal Reading 1Ketherin LeeNo ratings yet
- Forensic Odontology 3Document6 pagesForensic Odontology 3latifah hannumNo ratings yet
- Patient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionDocument9 pagesPatient Satisfaction Following Orthognathic Surgical Correction of Skeletal Class III MalocclusionAbles227 BlessNo ratings yet
- LBM 6 Blok 20 SGD 1Document8 pagesLBM 6 Blok 20 SGD 1Ani LabibahNo ratings yet
- 6 - Effects of Twin Block Vs Sagittal Guidance 2Document11 pages6 - Effects of Twin Block Vs Sagittal Guidance 2gnan.rebelNo ratings yet
- Aparicio C. Periodontology 2000Document19 pagesAparicio C. Periodontology 2000Luis Alberto Carpio MorenoNo ratings yet
- RCT FinalDocument13 pagesRCT FinalDaniela NoreñaNo ratings yet
- Post MortemDocument4 pagesPost MortemErlinda YulyNo ratings yet
- Definitive Obturator Modified For Crown - PPTX DR AmrDocument49 pagesDefinitive Obturator Modified For Crown - PPTX DR AmrHatem Ibrahim Ahmed AburiaNo ratings yet
- Layering and Curing Techniques For Class III Restorations: A Two-Year CaseDocument10 pagesLayering and Curing Techniques For Class III Restorations: A Two-Year CasetsukiyaNo ratings yet
- The Daughter Test in Aesthetic or Cosmetic DentiDocument8 pagesThe Daughter Test in Aesthetic or Cosmetic DentiRay ChaoNo ratings yet
- FFG Are Contraindications For Classes I and IIDocument8 pagesFFG Are Contraindications For Classes I and IIChin GeslaniNo ratings yet
- Glossary of Orthodontic TermsDocument6 pagesGlossary of Orthodontic TermsRohan John MichaelNo ratings yet
- Moraes 2009Document7 pagesMoraes 2009Gifix GifunNo ratings yet
- SR Phonares II Tooth Mould ChartDocument8 pagesSR Phonares II Tooth Mould ChartSomnath SenguptaNo ratings yet
- Vailati Masterclass: Course Program ITDocument13 pagesVailati Masterclass: Course Program ITItalo TorresNo ratings yet
- Njopeka AN, Mwangosi IEAT: Original ArticleDocument6 pagesNjopeka AN, Mwangosi IEAT: Original ArticleTôn Thất Đam TriềuNo ratings yet
- Dental Clinic Database SystemDocument23 pagesDental Clinic Database SystemTha Ita68% (22)
- The Efficacy of Maxillary Protraction Protocols With The Micro Implant Assisted Rapid Palatal Expander Marpe and The Novel n2 Mini Implant A Finite Element StudyDocument14 pagesThe Efficacy of Maxillary Protraction Protocols With The Micro Implant Assisted Rapid Palatal Expander Marpe and The Novel n2 Mini Implant A Finite Element StudySam PrasanthNo ratings yet
- Jurnal Askegilut PDFDocument6 pagesJurnal Askegilut PDFPutri Mayang Sari gigiNo ratings yet
- The Injection Resin Technique A Novel ConceptDocument15 pagesThe Injection Resin Technique A Novel ConceptJuan Francisco CamposNo ratings yet
- OrthodonticPracticeUS MayJunedigitalDocument64 pagesOrthodonticPracticeUS MayJunedigitalJuanNo ratings yet
- BooksDocument3 pagesBooksPurva JingarNo ratings yet
- Int Endodontic J - 2020 - Silva - Current Status On Minimal Access Cavity Preparations A Critical Analysis and A ProposalDocument18 pagesInt Endodontic J - 2020 - Silva - Current Status On Minimal Access Cavity Preparations A Critical Analysis and A ProposalPhương Thanh HoàngNo ratings yet
- 020 Over DenturesDocument60 pages020 Over DenturesKhan MustafaNo ratings yet
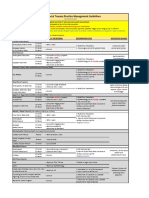
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- Etiology of MalocclusionDocument48 pagesEtiology of MalocclusionGilani Syed Sohaib100% (1)
- Atypical Developmental Defects of Enamel in Primary Incisors Versus Preeruptive Intracoronal Resorption (PEIR) : Case ReportsDocument4 pagesAtypical Developmental Defects of Enamel in Primary Incisors Versus Preeruptive Intracoronal Resorption (PEIR) : Case ReportsElizabeth CortésNo ratings yet
- Ijomi 15 415Document4 pagesIjomi 15 415Bagis Emre GulNo ratings yet
- Fornemc 15111Document98 pagesFornemc 15111Vanshika SethiNo ratings yet