You might also like
- Part 2 - MEDTERM-117 LECDocument9 pagesPart 2 - MEDTERM-117 LECfrechel kimNo ratings yet
- 11 Chemical Co-Ordination N Integration-Notes Blog (Full Permission)Document3 pages11 Chemical Co-Ordination N Integration-Notes Blog (Full Permission)fariha khanNo ratings yet
- DwarfismDocument5 pagesDwarfismjasminemuammilNo ratings yet
- Endocrine System Physiology and Pathophysiology (Part 1)Document34 pagesEndocrine System Physiology and Pathophysiology (Part 1)ayaessam392002No ratings yet
- 22. Chemical Co Ordination and Integration_434dea34 f494 4704 a8c9 6876397e324eDocument53 pages22. Chemical Co Ordination and Integration_434dea34 f494 4704 a8c9 6876397e324epcgurukotari9No ratings yet
- Pituitary Gland DisordersDocument80 pagesPituitary Gland DisordersNang KhamNo ratings yet
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocument22 pagesAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiNo ratings yet
- Anterior Pituitary GlandDocument29 pagesAnterior Pituitary GlandSyed Mohammad Osama AhsanNo ratings yet
- Diseases of Endocrine GlandsDocument3 pagesDiseases of Endocrine GlandsSamantha Dasmariñas MagaanNo ratings yet
- Pituitary Hormones and Their FunctionsDocument8 pagesPituitary Hormones and Their FunctionsNoreen B. BañagadoNo ratings yet
- PNKND Les 0 V 9 VWR60 B RCNDocument4 pagesPNKND Les 0 V 9 VWR60 B RCNaadeshthite476No ratings yet
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDocument27 pagesThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanNo ratings yet
- ENDOCRINE NURSING-FINAL HDDocument15 pagesENDOCRINE NURSING-FINAL HDJayvee Novenario Casaljay100% (1)
- Endocrine - BoardsDocument9 pagesEndocrine - BoardsSoojung Nam100% (4)
- Endocrine System: Practical PartDocument58 pagesEndocrine System: Practical PartAmy AmyNo ratings yet
- Hormonal Disorders and Their CausesDocument12 pagesHormonal Disorders and Their CausesRK YeleswarapuNo ratings yet
- Micropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyDocument4 pagesMicropenis or Cryptorchidism Kallman's Syndrome:: Thyroid-Stimulating (TSH) DeficiencyYessamin Paith RoderosNo ratings yet
- 2023 Med SurgDocument87 pages2023 Med Surgkhaidkhan0609No ratings yet
- Dr. Methaq A.M.Hussein: MRCP (London) ,,sce of Endocrine (London) FIBIMS, Professor of Medicine LECT. 1,2Document8 pagesDr. Methaq A.M.Hussein: MRCP (London) ,,sce of Endocrine (London) FIBIMS, Professor of Medicine LECT. 1,2hussain AltaherNo ratings yet
- What Is Addison's Disease Cause Symptoms: Low Blood Pressure HyperpigmentationDocument8 pagesWhat Is Addison's Disease Cause Symptoms: Low Blood Pressure HyperpigmentationMd FameeNo ratings yet
- 22 Chemical Co-OrdinationDocument47 pages22 Chemical Co-OrdinationRachna JaiswalNo ratings yet
- Endocrinology: Elizabeth H., MD. PathologistDocument72 pagesEndocrinology: Elizabeth H., MD. PathologistABUBEKER BESHIRNo ratings yet
- ArainDocument71 pagesArainAllah Bux KhosoNo ratings yet
- Endocrine Glands and Their FunctionsDocument31 pagesEndocrine Glands and Their FunctionsAfrina Asmi MINo ratings yet
- Approach To Short StatureDocument71 pagesApproach To Short StatureOmar HamwiNo ratings yet
- MODULE 2 Disorders of The Pituitary GlandDocument24 pagesMODULE 2 Disorders of The Pituitary GlandLorraine GambitoNo ratings yet
- Pituitary PathologyDocument5 pagesPituitary PathologyNada MuchNo ratings yet
- Inbound 5293281166643491950Document15 pagesInbound 5293281166643491950MUHAMMAD ISHAQNo ratings yet
- SEMINAR ON PITUITARY DISORDERS PRESENTED BY ZORINSANGIDocument62 pagesSEMINAR ON PITUITARY DISORDERS PRESENTED BY ZORINSANGIZorini ChhangteNo ratings yet
- The Endocrine SystemDocument3 pagesThe Endocrine Systemheyraheyra70No ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemYary MayorNo ratings yet
- Hypothyroidism: By: Judhaimah Mardhiah BT Mat Tari 0810544Document23 pagesHypothyroidism: By: Judhaimah Mardhiah BT Mat Tari 0810544Jujue MardhiahNo ratings yet
- Endocrine NotesDocument1 pageEndocrine NotesShivraj singh RajputNo ratings yet
- Path Endocrine OutlineDocument46 pagesPath Endocrine Outlineaya derweshNo ratings yet
- Thyroid DisordersDocument61 pagesThyroid DisordersdrmamodoNo ratings yet
- Lecture.11 Endocrine System 1Document43 pagesLecture.11 Endocrine System 1Mohammed AlaaNo ratings yet
- Chemical Coordination and IntegrationDocument3 pagesChemical Coordination and Integrationakhil01ajNo ratings yet
- 2 Pitutary GlandDocument44 pages2 Pitutary GlandHanen ZedanNo ratings yet
- Dr.Rihab Pediatrics 04.HypothyroidismDocument7 pagesDr.Rihab Pediatrics 04.HypothyroidismMujtaba JawadNo ratings yet
- HyperpituitarismDocument2 pagesHyperpituitarismsaba969_No ratings yet
- Endocrine: - o in Males It Induces Sexual ArousalDocument32 pagesEndocrine: - o in Males It Induces Sexual ArousalEmily CarlsonNo ratings yet
- Lecture 7Document8 pagesLecture 7hossam369No ratings yet
- Pituitary DisorderDocument48 pagesPituitary DisorderAyumi AgungNo ratings yet
- Chapter 5 - The Endocrine System - FinalDocument57 pagesChapter 5 - The Endocrine System - FinalKharrel YballeNo ratings yet
- Essentials of Anatomy & Physiology: The Endocrine SystemDocument52 pagesEssentials of Anatomy & Physiology: The Endocrine SystemMarrenSalvadorNo ratings yet
- Pituitary Tumors (Adenoma, Craniopharyngioma)Document6 pagesPituitary Tumors (Adenoma, Craniopharyngioma)Ram RamNo ratings yet
- PBL Week 1 Jumat EndocrineDocument29 pagesPBL Week 1 Jumat EndocrineHelena PadilahNo ratings yet
- #4 Hypothalamic & Pituitary Hormones 7 PDFDocument7 pages#4 Hypothalamic & Pituitary Hormones 7 PDFOmar BasimNo ratings yet
- Levels of Calcium in Your Blood To Rise, A Condition Known As Hypercalcemia)Document3 pagesLevels of Calcium in Your Blood To Rise, A Condition Known As Hypercalcemia)Pandesal with EggNo ratings yet
- Levels of Calcium in Your Blood To Rise, A Condition Known As Hypercalcemia)Document3 pagesLevels of Calcium in Your Blood To Rise, A Condition Known As Hypercalcemia)Pandesal with EggNo ratings yet
- Endocrine System Animal ScienceDocument15 pagesEndocrine System Animal ScienceJairus LampanoNo ratings yet
- Nursing Care for Children with Endocrine and Metabolic DisordersDocument22 pagesNursing Care for Children with Endocrine and Metabolic DisordersAlyssaGrandeMontimorNo ratings yet
- Untitled PresentationDocument8 pagesUntitled Presentationkymanidouglas06No ratings yet
- Endocrine System GuideDocument21 pagesEndocrine System GuidePete Cobra CobraitiNo ratings yet
- Dermatologic manifestations of hypopituitarismDocument10 pagesDermatologic manifestations of hypopituitarismWPRN RanasingheNo ratings yet
- Pathophysiology of The Endocrine System. Violation of Hypophysis, Thyroid and Adrenal Glands. General Adaptation SyndromeDocument123 pagesPathophysiology of The Endocrine System. Violation of Hypophysis, Thyroid and Adrenal Glands. General Adaptation SyndromeAyman RehmanNo ratings yet
- Hormones: Resmia A. MaulanaDocument42 pagesHormones: Resmia A. MaulanaCanny CańasNo ratings yet
- HypothyroidismDocument49 pagesHypothyroidismBahaa ShaabanNo ratings yet
- Hypopituitarism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypopituitarism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemEthel May AlabastroNo ratings yet
- Drugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdDocument22 pagesDrugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdRtxGaming Zone 73No ratings yet
- Plab 1 Lectures Endo NotesDocument81 pagesPlab 1 Lectures Endo NotesmesutNo ratings yet
- Zaina PDFDocument1 pageZaina PDFZaina AkramNo ratings yet
- Unit IV Lecture NotesDocument9 pagesUnit IV Lecture NotesSteve SullivanNo ratings yet
- InfertilityDocument10 pagesInfertilityHarish Labana100% (1)
- Insulin PharmacologyDocument1 pageInsulin PharmacologyzainabNo ratings yet
- Percutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookDocument20 pagesPercutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookRanda TabbahNo ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- BB Glow TreatmentDocument19 pagesBB Glow TreatmentDrAmit Gaba MdsNo ratings yet
- Polycystic Ovary SyndromeDocument19 pagesPolycystic Ovary SyndromeJalal AlbadriNo ratings yet
- Hypoglycemia: 8 TermDocument45 pagesHypoglycemia: 8 Termswathi bs100% (1)
- Test report for thyroid profile of Mr. N Hemanth KumarDocument1 pageTest report for thyroid profile of Mr. N Hemanth KumarN Hemanth KumarNo ratings yet
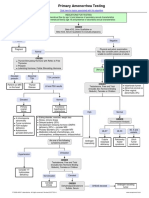
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Fasting in The Treatment of Diabetes and High Blood PressureDocument2 pagesFasting in The Treatment of Diabetes and High Blood PressureTrueNorth Health Center100% (1)
- HypothalamusDocument38 pagesHypothalamuscmabdullahNo ratings yet
- UNIT II Endocrine & Metabolic DisordersDocument19 pagesUNIT II Endocrine & Metabolic DisordersAmmar BhattiNo ratings yet
- Gastro-Intestinal Hormones & TransmittersDocument23 pagesGastro-Intestinal Hormones & TransmittersAlbert ChuwaNo ratings yet
- A Review of GrowthDocument8 pagesA Review of GrowthEmilia Diana IacobNo ratings yet
- 2014 IMSO Science KeysDocument10 pages2014 IMSO Science KeysThanh DinhNo ratings yet
- Govind AmbiGen PosterDocument1 pageGovind AmbiGen PosterYolanda MNo ratings yet
- Commercial Production of HormonesDocument2 pagesCommercial Production of HormonessumayyaNo ratings yet
- Diabetes Management & Insulin InitiationDocument39 pagesDiabetes Management & Insulin InitiationTaufiqurrochman Nur AminNo ratings yet
- Case Discussion on Polycystic Ovarian SyndromeDocument55 pagesCase Discussion on Polycystic Ovarian SyndromeGenevie Ombao100% (1)
- Relationship Between Body SystemsDocument2 pagesRelationship Between Body SystemsG8 Akshita BiswasNo ratings yet
- Disorders of Sodium and Potassium MetabolismDocument18 pagesDisorders of Sodium and Potassium MetabolismTukuWoNo ratings yet
- Nurse Review: Medical-Surgical Nursing Endocrine System 2005Document215 pagesNurse Review: Medical-Surgical Nursing Endocrine System 2005jonas2663No ratings yet
- Immulite Assay Menu PDFDocument2 pagesImmulite Assay Menu PDFОлександрNo ratings yet
- Test Bank For Nutrition Through The Life Cycle 5th Edition Judith e BrownDocument36 pagesTest Bank For Nutrition Through The Life Cycle 5th Edition Judith e Brownmyositisenigmakoh3100% (43)
- Female Infertility - Causes - UpToDateDocument13 pagesFemale Infertility - Causes - UpToDateTaís CidrãoNo ratings yet