You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
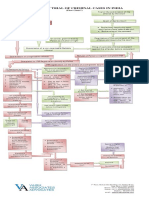
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Design Engineering JourneyDocument159 pagesDesign Engineering JourneyKarenNo ratings yet
- 39 Storey Treehouse Activity Pack PDFDocument11 pages39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Christian Borch & Gernot Bohme & Olafur Eliasson & Juhani Pallasmaa - Architectural Atmospheres-BirkhauserDocument112 pagesChristian Borch & Gernot Bohme & Olafur Eliasson & Juhani Pallasmaa - Architectural Atmospheres-BirkhauserAja100% (1)
- Ceftriaxone: Skip To Main ContentDocument44 pagesCeftriaxone: Skip To Main ContentHandayaniNo ratings yet
- NYERI - Aplikasi DinginDocument7 pagesNYERI - Aplikasi DinginHandayaniNo ratings yet
- PublishedVersion COR2-17014719Document16 pagesPublishedVersion COR2-17014719HandayaniNo ratings yet
- 825 1733 1 PBDocument9 pages825 1733 1 PBHandayaniNo ratings yet
- Nihms 1645342Document16 pagesNihms 1645342HandayaniNo ratings yet
- Nyeri - Titik HugoDocument6 pagesNyeri - Titik HugoHandayaniNo ratings yet
- NYERI DistractionDocument6 pagesNYERI DistractionHandayaniNo ratings yet
- 1 s2.0 S2772368222000130 MainDocument23 pages1 s2.0 S2772368222000130 MainHandayaniNo ratings yet
- Evaluation of A Potential Clinical Interaction BetDocument8 pagesEvaluation of A Potential Clinical Interaction BetHandayaniNo ratings yet
- NYERI ReligiusDocument9 pagesNYERI ReligiusHandayaniNo ratings yet
- Burns: Pathophysiology of Systemic Complications and Current ManagementDocument13 pagesBurns: Pathophysiology of Systemic Complications and Current ManagementHandayaniNo ratings yet
- Continuing Education Activity: Hemorrhagic StrokeDocument18 pagesContinuing Education Activity: Hemorrhagic StrokeHandayaniNo ratings yet
- Perioperative Hypothermia-A Narrative Review: Environmental Research and Public HealthDocument15 pagesPerioperative Hypothermia-A Narrative Review: Environmental Research and Public HealthHandayaniNo ratings yet
- Struzik 2019Document5 pagesStruzik 2019HandayaniNo ratings yet
- The 2020 WHO Classification: What 'S New in Soft Tissue Tumor Pathology?Document23 pagesThe 2020 WHO Classification: What 'S New in Soft Tissue Tumor Pathology?HandayaniNo ratings yet
- Thermal Homeostasis in The Newborn Puppy: Behavioral and Physiological ResponsesDocument12 pagesThermal Homeostasis in The Newborn Puppy: Behavioral and Physiological ResponsesHandayaniNo ratings yet
- To The Operating Room! Positive Effects of A Healthcare Clown Intervention On Children Undergoing SurgeryDocument13 pagesTo The Operating Room! Positive Effects of A Healthcare Clown Intervention On Children Undergoing SurgeryHandayaniNo ratings yet
- Continuing Education Activity: Pneumonia PathologyDocument14 pagesContinuing Education Activity: Pneumonia PathologyHandayaniNo ratings yet
- Common Cold in Children-I: Diagnosis: October 2019Document9 pagesCommon Cold in Children-I: Diagnosis: October 2019HandayaniNo ratings yet
- Effectiveness of Antenatal Nursing Intervention On Childbirth's Fears, Psychological-Wellbeing and Pregnancy Outcomes in Primipara's WomenDocument9 pagesEffectiveness of Antenatal Nursing Intervention On Childbirth's Fears, Psychological-Wellbeing and Pregnancy Outcomes in Primipara's WomenHandayaniNo ratings yet
- Malaria in Early Life 2Document15 pagesMalaria in Early Life 2HandayaniNo ratings yet
- Gastroent 09 06665Document3 pagesGastroent 09 06665HandayaniNo ratings yet
- COT Cott Aug 2017Document30 pagesCOT Cott Aug 2017Ala BasterNo ratings yet
- D245S 734046 Om enDocument90 pagesD245S 734046 Om enEndro Accoustic100% (1)
- Core Values Revised 3Document4 pagesCore Values Revised 3api-457909911No ratings yet
- Chap5-7 National Book Foundation 9th Class Conceptual QuestionsDocument7 pagesChap5-7 National Book Foundation 9th Class Conceptual QuestionsWaleed Nasir100% (1)
- By John Chaffee: Thinking CriticallyDocument6 pagesBy John Chaffee: Thinking CriticallygeoedukoreaNo ratings yet
- Allergens 08242023Document5 pagesAllergens 08242023Maalvika SinghNo ratings yet
- 7 Types of English Adjectives That Every ESL Student Must KnowDocument3 pages7 Types of English Adjectives That Every ESL Student Must KnowBenny James CloresNo ratings yet
- Indefinite and Definite ArticlesDocument19 pagesIndefinite and Definite ArticlesRantti AnwarNo ratings yet
- MVP Teacher 12Document6 pagesMVP Teacher 12Ivan ChuNo ratings yet
- AIKINS v. KOMMENDADocument6 pagesAIKINS v. KOMMENDAMENSAH PAULNo ratings yet
- Adverbial Phrases 3Document21 pagesAdverbial Phrases 3Jobelle VergaraNo ratings yet
- Bow Thruster CatalogLRDocument28 pagesBow Thruster CatalogLRAlexey RulevskiyNo ratings yet
- Fig. 6.14 Circular WaveguideDocument16 pagesFig. 6.14 Circular WaveguideThiagu RajivNo ratings yet
- Grade 5 DLL ENGLISH 5 Q3 Week 2Document7 pagesGrade 5 DLL ENGLISH 5 Q3 Week 2Armie Joimie ValdezNo ratings yet
- Fashion Designer Research Paper ThesisDocument4 pagesFashion Designer Research Paper Thesisafbteyrma100% (2)
- Events ProposalsDocument19 pagesEvents ProposalsRam-tech Jackolito FernandezNo ratings yet
- Prgm-Sminr Faculties Identified Through FIP NIRCDocument9 pagesPrgm-Sminr Faculties Identified Through FIP NIRCDonor CrewNo ratings yet
- Sara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementDocument6 pagesSara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementKeerthi PurushothamanNo ratings yet
- Indian RailwaysDocument20 pagesIndian RailwaysNirmalNo ratings yet
- Financial Fitness ChecklistDocument4 pagesFinancial Fitness Checklistcoach_22No ratings yet
- Stock Market Prediction Using Machine Learning ProposalDocument10 pagesStock Market Prediction Using Machine Learning ProposalBilal AhmedNo ratings yet
- Easy Trade Manager Forex RobotDocument10 pagesEasy Trade Manager Forex RobotPinda DhanoyaNo ratings yet
- Wollo UniversityDocument14 pagesWollo UniversityabdishakurNo ratings yet
- Assignment 1684490923Document16 pagesAssignment 1684490923neha.engg45755No ratings yet
- English Full Book PaperDocument2 pagesEnglish Full Book PaperSaira BatoolNo ratings yet
- Knock Knock GamesDocument1 pageKnock Knock GamesArsyta AnandaNo ratings yet