You might also like
- The Bucegi Mountain !Document169 pagesThe Bucegi Mountain !NormanNo ratings yet
- Finishing & DetailingDocument28 pagesFinishing & DetailingBikramjeet Singh100% (4)
- Retention and Relapse SeminarDocument51 pagesRetention and Relapse SeminarShabeel Pn100% (2)
- Orthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportDocument3 pagesOrthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportEditor IJTSRDNo ratings yet
- MBT 2Document11 pagesMBT 2NaveenNo ratings yet
- Surgical OrthodonticsDocument5 pagesSurgical OrthodonticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Beggs Philosophy Ortho / Orthodontic Courses by Indian Dental AcademyDocument81 pagesBeggs Philosophy Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- MBTDocument65 pagesMBTdangi.ishu29No ratings yet
- Watchtower: Talk Outline, How Well Do You Know God?Document1 pageWatchtower: Talk Outline, How Well Do You Know God?sirjsslut100% (1)
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Centre of Resistance of MaxillaDocument2 pagesCentre of Resistance of MaxillasameerorthoNo ratings yet
- Opus LoopDocument9 pagesOpus LoopMuhammad AsimNo ratings yet
- Clinical Photography in OrthodonticsDocument5 pagesClinical Photography in OrthodonticsRocio100% (2)
- Loops and RetractionDocument24 pagesLoops and RetractionYuvashreeNo ratings yet
- Begg's and Tip Edge PhilosophyDocument74 pagesBegg's and Tip Edge PhilosophyNeel Lalmani MauryaNo ratings yet
- TorqueDocument12 pagesTorqueTamkeen FarahNo ratings yet
- Biomechanics of Deep Bite TreatmentDocument66 pagesBiomechanics of Deep Bite TreatmentMaitreye PriyadarshiniNo ratings yet
- English Worksheets. Unit 1 2 6 7 8Document4 pagesEnglish Worksheets. Unit 1 2 6 7 8Paula Seijas GonzálezNo ratings yet
- Space Closure Using Frictionless MechanicsDocument11 pagesSpace Closure Using Frictionless MechanicsLisbethNo ratings yet
- V-Bend and Anchorage in Orthodontics: Mehak Arya Iyrmds Dept of OrthodonticsDocument37 pagesV-Bend and Anchorage in Orthodontics: Mehak Arya Iyrmds Dept of OrthodonticsMehak AryaNo ratings yet
- Syllabus Transportation Law (Sucgang) Part1Document6 pagesSyllabus Transportation Law (Sucgang) Part1Ruby Santillana100% (1)
- Extraction Vs Non Extraction Controversy: A Review: January 2018Document9 pagesExtraction Vs Non Extraction Controversy: A Review: January 2018Jawad TariqNo ratings yet
- Friction in OrthodonticsDocument71 pagesFriction in OrthodonticsNimisha SharmaNo ratings yet
- Intrusion Arches ShinuDocument66 pagesIntrusion Arches ShinuYuvashreeNo ratings yet
- Curing Lights in OrthodonticsDocument31 pagesCuring Lights in OrthodonticsPerthish sharmaNo ratings yet
- Skeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealityDocument10 pagesSkeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealitySoe San KyawNo ratings yet
- A Study of Service Quality, Customer Satisfaction, Corporate Image and Customer Loyalty in The Hotel Industry in MalaysiaDocument20 pagesA Study of Service Quality, Customer Satisfaction, Corporate Image and Customer Loyalty in The Hotel Industry in MalaysiaVic Chong0% (1)
- Journal of Oral Health & DentistryDocument6 pagesJournal of Oral Health & DentistryFernando Caro PinillaNo ratings yet
- Comparative Study of Idealism, Naturalism, Pragmatism & RealismDocument5 pagesComparative Study of Idealism, Naturalism, Pragmatism & RealismAnjali DasNo ratings yet
- Introduction To Montessori Education0001 PDFDocument5 pagesIntroduction To Montessori Education0001 PDFFatushe JasharajNo ratings yet
- 1.self Ligating Brackets Past Present Future of OrthodonticsDocument5 pages1.self Ligating Brackets Past Present Future of OrthodonticsFrancisco Vega GarciaNo ratings yet
- Orthodontic Root Resorption: Abhijeet JaiswalDocument56 pagesOrthodontic Root Resorption: Abhijeet JaiswalDr.Sakshi katyalNo ratings yet
- Dendera Light BulbDocument16 pagesDendera Light BulbNabil Roufail50% (2)
- The Cult of UnschoolingDocument9 pagesThe Cult of UnschoolingJon Gold100% (2)
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- 018 Vs 022Document3 pages018 Vs 022kkorina5100% (2)
- 36 Canine Retraction in Orthodontics - A Review of Various MethodsDocument9 pages36 Canine Retraction in Orthodontics - A Review of Various MethodsRahma Wahid100% (1)
- Creekmore1993 1 PDFDocument13 pagesCreekmore1993 1 PDFsmritiNo ratings yet
- The Butter y System: Brackets, Prescription, and AuxiliariesDocument9 pagesThe Butter y System: Brackets, Prescription, and AuxiliariesNonoNo ratings yet
- Occlusion - DevelopmentDocument33 pagesOcclusion - Developmentsameerortho100% (1)
- Biomechanics of Deep Overbite CorrectionDocument8 pagesBiomechanics of Deep Overbite CorrectionLuis Paipay SantosNo ratings yet
- Evaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDocument6 pagesEvaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDiana Paola FontechaNo ratings yet
- Diagnostic Elements For Tooth Extraction in OrthodonticsDocument24 pagesDiagnostic Elements For Tooth Extraction in OrthodonticsLanaNo ratings yet
- 1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneDocument35 pages1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneRockey ShrivastavaNo ratings yet
- One Couple SystemDocument13 pagesOne Couple Systemmanju deviNo ratings yet
- KLoop Molar Distalizing AppDocument7 pagesKLoop Molar Distalizing AppAngie Römer HaroNo ratings yet
- Biostatistics in OrthodonticsDocument117 pagesBiostatistics in OrthodonticsJoshua StalinNo ratings yet
- Journal Club List Second Year Postgraduates: Department of Orthodontics and Dentofacial OrthopedicsDocument6 pagesJournal Club List Second Year Postgraduates: Department of Orthodontics and Dentofacial OrthopedicsMariyam0% (1)
- Scissors Bite-Dragon Helix ApplianceDocument6 pagesScissors Bite-Dragon Helix ApplianceGaurav PatelNo ratings yet
- Anchorage in OrthodonticsDocument123 pagesAnchorage in Orthodonticsdrimtiyaz123No ratings yet
- MANAGEMENT OF VERTICAL MAXILLARY EXCESS WWWDocument24 pagesMANAGEMENT OF VERTICAL MAXILLARY EXCESS WWWsweetieNo ratings yet
- Ortho ScarsDocument6 pagesOrtho ScarssandeepNo ratings yet
- Newer Orthodontic Arch WiresDocument81 pagesNewer Orthodontic Arch WiresMothi Krishna100% (1)
- Adult Transverse Diagnosis and Treatment A Case Ba - 2019 - Seminars in OrthodoDocument40 pagesAdult Transverse Diagnosis and Treatment A Case Ba - 2019 - Seminars in OrthodoOmy J. Cruz100% (1)
- Pedagogy Torqunig AuxillariesDocument39 pagesPedagogy Torqunig AuxillariesGudiyA KaurNo ratings yet
- Customized BracketsDocument69 pagesCustomized BracketssakshiNo ratings yet
- Vari-Simplex DisciplineDocument60 pagesVari-Simplex DisciplineDrGurinder Kanwar100% (1)
- The 2 X 4 Appliance McKeown SandlerDocument4 pagesThe 2 X 4 Appliance McKeown Sandlervefiisphepy83312No ratings yet
- A Dilemma in Orthodontics Extractions in Borderline CasesDocument4 pagesA Dilemma in Orthodontics Extractions in Borderline CasesOsama MohamedNo ratings yet
- Cast AnalysisDocument9 pagesCast AnalysisAhmed SharabyNo ratings yet
- Attachments & Auxiliaries in Begg's TechniqueDocument117 pagesAttachments & Auxiliaries in Begg's TechniqueswapniljunnarkarNo ratings yet
- Arch Forms 1-Ortho / Orthodontic Courses by Indian Dental AcademyDocument48 pagesArch Forms 1-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- !excellence in Finishing Current Concepts Goals and Mechanics PDFDocument13 pages!excellence in Finishing Current Concepts Goals and Mechanics PDFMargarita Lopez Martinez100% (1)
- Functional Occlusion in Orthodontics: ClinicalDocument11 pagesFunctional Occlusion in Orthodontics: ClinicalNaeem MoollaNo ratings yet
- Growth PredictionDocument64 pagesGrowth PredictionMothi KrishnaNo ratings yet
- Theories in NursingDocument22 pagesTheories in NursingChrisgr8No ratings yet
- Call +91 9712985389: To Enquire. Whatsapp: 9830110214Document15 pagesCall +91 9712985389: To Enquire. Whatsapp: 9830110214ThomDeltaNo ratings yet
- Entity Relationship Diagram Notes - BBADocument15 pagesEntity Relationship Diagram Notes - BBAAshish PaswanNo ratings yet
- DISCUSSION 2 - Film TheoriesDocument3 pagesDISCUSSION 2 - Film TheoriesKenn SolomonNo ratings yet
- Script Writing PRTDocument3 pagesScript Writing PRTLena HannaNo ratings yet
- Ek Ruka Hua FaislaDocument3 pagesEk Ruka Hua FaislaRaju Mahato100% (1)
- 2001 Sturtevant A History of GeneticsDocument179 pages2001 Sturtevant A History of Geneticsmabru_blackNo ratings yet
- Policymaking For Human Enhancement Technologies: Scientific Description, Philosophical Prescription, and The Constraints of Law, Hannah MaslenDocument15 pagesPolicymaking For Human Enhancement Technologies: Scientific Description, Philosophical Prescription, and The Constraints of Law, Hannah MaslenJournal of Law, Information & ScienceNo ratings yet
- Observation Sheet - Questioning: Question TypeDocument7 pagesObservation Sheet - Questioning: Question Typeapi-372535556No ratings yet
- CS402 FULL Material 2011Document271 pagesCS402 FULL Material 2011Muhammad Ali100% (1)
- Relationship Essay: Sample IntroductionDocument7 pagesRelationship Essay: Sample IntroductionnelsonNo ratings yet
- Aristotle's RevengeDocument9 pagesAristotle's Revengebridgetmacgabhann0% (1)
- Workbook Answers: AS/A-level English Literature WorkbookDocument42 pagesWorkbook Answers: AS/A-level English Literature WorkbooktelmarventuraNo ratings yet
- The PoemDocument14 pagesThe PoemAisley ChrimsonNo ratings yet
- Rotational Motion Part-BDocument25 pagesRotational Motion Part-Bsmi_santhosh100% (1)
- Types of FamilyDocument4 pagesTypes of FamilyGarry Camposano YutucNo ratings yet
- Reaching For Common Ground in K-12 Mathematics EducationDocument4 pagesReaching For Common Ground in K-12 Mathematics EducationAndrew CourtneyNo ratings yet
- MEd SB G02 en 04-Oct DigitalDocument96 pagesMEd SB G02 en 04-Oct DigitalNishana Shajahan0% (1)
- Zenit & Expo PDFDocument5 pagesZenit & Expo PDFVagueBlurNo ratings yet
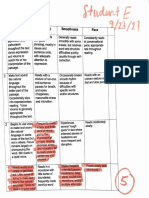
- Multidimensional Fluency Scale Rubric 1Document1 pageMultidimensional Fluency Scale Rubric 1api-548626684No ratings yet
- Florine and Maria Cambridge English First Fce From 2015 Speaking Test VideoDocument5 pagesFlorine and Maria Cambridge English First Fce From 2015 Speaking Test VideoJ Christian OdehnalNo ratings yet