You might also like
- BLS Acls Aha 2020Document103 pagesBLS Acls Aha 2020Nicholas PetrovskiNo ratings yet
- POTS Current Concepts Trends in CVMDocument5 pagesPOTS Current Concepts Trends in CVMmperlethNo ratings yet
- Sugar Free Shopping ListDocument4 pagesSugar Free Shopping Listhsquiers100% (3)
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- Cerebral Oxygenation and The Recoverable BrainDocument4 pagesCerebral Oxygenation and The Recoverable BrainThumiso MasohaNo ratings yet
- Understanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFDocument11 pagesUnderstanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFMihaela BalionNo ratings yet
- Notes On Critical Areas in Labor Law Part IiDocument66 pagesNotes On Critical Areas in Labor Law Part IipaulNo ratings yet
- JUVENILE Justice ProjectDocument24 pagesJUVENILE Justice ProjectyashaNo ratings yet
- The Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureDocument10 pagesThe Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureadeNo ratings yet
- Mechanisms of Cardiovascular Homeostasis and Pathophysiology Expression, Signal Transduction To Cellular CommunicationDocument2 pagesMechanisms of Cardiovascular Homeostasis and Pathophysiology Expression, Signal Transduction To Cellular CommunicationRyan Carlo CondeNo ratings yet
- Editorial: Pathogenesis of Heart Failure Xi: Jagat Narula and James B. YoungDocument4 pagesEditorial: Pathogenesis of Heart Failure Xi: Jagat Narula and James B. YoungantothesaberNo ratings yet
- Pathogenesis of Hepatic Encephalopathy in Acute Liver Failure 2003Document12 pagesPathogenesis of Hepatic Encephalopathy in Acute Liver Failure 2003MarleyNo ratings yet
- Neurological Complications After Cardiac Surgery4401Document13 pagesNeurological Complications After Cardiac Surgery4401Dewa BraÇika Damma PrasadaNo ratings yet
- Pathogenesis and Clinical Presentation of Acute Heart FailureDocument7 pagesPathogenesis and Clinical Presentation of Acute Heart FailureNICOLAS ESTEBAN PARDO DIAZNo ratings yet
- 9 Case Report-HyponatremiaDocument2 pages9 Case Report-HyponatremiaKamal Kumar Kamal KumarNo ratings yet
- Evolving Indications For Permanent PacemakersDocument12 pagesEvolving Indications For Permanent PacemakersJazmín Alejandra AGNo ratings yet
- Mitchell 2005Document8 pagesMitchell 2005DianNo ratings yet
- Optimal PH Strategy For Hypothermic Circulatory Ar PDFDocument2 pagesOptimal PH Strategy For Hypothermic Circulatory Ar PDFKhairunnisa FitriNo ratings yet
- Francis 2001Document10 pagesFrancis 2001HnWishNo ratings yet
- Clinical Cardiology - 2009 - Colucci - The Effects of Norepinephrine On Myocardial Biology Implications For The Therapy ofDocument5 pagesClinical Cardiology - 2009 - Colucci - The Effects of Norepinephrine On Myocardial Biology Implications For The Therapy ofkallolchakraborty779204No ratings yet
- Archneur 23 2 003Document7 pagesArchneur 23 2 003Robert JenkinsNo ratings yet
- Neuromodulation in Treatment of Hypertension by Acupuncture: A Neurophysiological ProspectiveDocument8 pagesNeuromodulation in Treatment of Hypertension by Acupuncture: A Neurophysiological Prospectivewillv4No ratings yet
- Food and Sustainability Full ChapterDocument23 pagesFood and Sustainability Full Chapterandrea.woodard222100% (27)
- Overview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyDocument3 pagesOverview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyTemesgen EndalewNo ratings yet
- Neurohormonal Hypothesis in Heart FailureDocument11 pagesNeurohormonal Hypothesis in Heart FailureCypress Trixia Mananquil MacapagalNo ratings yet
- Pathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Document17 pagesPathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Idha ANo ratings yet
- Basic Principles of Cerebral Protection in Humans: William L. LanierDocument4 pagesBasic Principles of Cerebral Protection in Humans: William L. Lanierrachel0301No ratings yet
- Melikian 2009Document7 pagesMelikian 2009atif shariqNo ratings yet
- 1 s2.0 S2452302X21003648 MainDocument29 pages1 s2.0 S2452302X21003648 MainMahdi HosseiniNo ratings yet
- 2008 2 92 PDFDocument8 pages2008 2 92 PDFdidiNo ratings yet
- Heart Disease IVDocument10 pagesHeart Disease IVJOUBERT ALVAREZNo ratings yet
- 10 1 1 278 5572 PDFDocument7 pages10 1 1 278 5572 PDFAnggelia jopa sariNo ratings yet
- Mineralocorticoid Receptor Activation and AntagoniDocument8 pagesMineralocorticoid Receptor Activation and AntagoniStivoNo ratings yet
- Review Article: A Review of The Pathophysiology and Novel Treatments For Erectile DysfunctionDocument10 pagesReview Article: A Review of The Pathophysiology and Novel Treatments For Erectile DysfunctionsasNo ratings yet
- Se FisiopatoDocument28 pagesSe Fisiopatocska398No ratings yet
- Cerebral Salt Wasting Syndrome ReviewDocument6 pagesCerebral Salt Wasting Syndrome ReviewSoewira Sastra100% (1)
- Astrocytes and Epilepsy: Nihal C. de Lanerolle, Tih-Shih Lee, and Dennis D. SpencerDocument15 pagesAstrocytes and Epilepsy: Nihal C. de Lanerolle, Tih-Shih Lee, and Dennis D. SpencerErsin KarataşNo ratings yet
- WFCCN Chapter 3 Shock and Multiple Organ Dysfunction 2nd-Edition EbookDocument53 pagesWFCCN Chapter 3 Shock and Multiple Organ Dysfunction 2nd-Edition EbookJuan Carlos Mora TorresNo ratings yet
- Camargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Document6 pagesCamargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Rizki Muhammad RanandaNo ratings yet
- 2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesDocument18 pages2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesConny MuñozNo ratings yet
- Imaging Consumption: PerfusionDocument3 pagesImaging Consumption: PerfusionDionisia Pipit SaraswatiNo ratings yet
- Paralisis de M.inferioresDocument2 pagesParalisis de M.inferioresHector Garcia LermaNo ratings yet
- ApneaDocument11 pagesApneagemelinesNo ratings yet
- Electrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNDocument4 pagesElectrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNchuck55No ratings yet
- Hypokalemic Periodic Paralysis A Case ReportDocument2 pagesHypokalemic Periodic Paralysis A Case ReportEditor IJTSRDNo ratings yet
- Mechanisms of Sympathoadrenal Failure and Hypoglycemia in DiabetesDocument4 pagesMechanisms of Sympathoadrenal Failure and Hypoglycemia in Diabetesfuna77No ratings yet
- Abstracts / Atherosclerosis 252 (2016) E1 Ee196 E185Document2 pagesAbstracts / Atherosclerosis 252 (2016) E1 Ee196 E185MaulNo ratings yet
- Controlled HypotensionDocument21 pagesControlled HypotensionChristian YonathanNo ratings yet
- Editorial: Now RateDocument6 pagesEditorial: Now RateDinka RoselyNo ratings yet
- Biomarkers of Volume Overload and Edema in HFDocument14 pagesBiomarkers of Volume Overload and Edema in HFalcasan63No ratings yet
- Cardiovascular Disease in AcromegalyDocument4 pagesCardiovascular Disease in AcromegalynissaNo ratings yet
- The Underlying Neurobiology of Bipolar Disorder: H K. M, J A. Q, J L. P, J S, B P. L, J S. V, C A. ZDocument11 pagesThe Underlying Neurobiology of Bipolar Disorder: H K. M, J A. Q, J L. P, J S, B P. L, J S. V, C A. ZRhodis PeñaNo ratings yet
- 10 1 1 622 7158 PDFDocument8 pages10 1 1 622 7158 PDFz31nNo ratings yet
- Cerebralsaltwasting: Pathophysiology, Diagnosis, and TreatmentDocument14 pagesCerebralsaltwasting: Pathophysiology, Diagnosis, and TreatmentCarinka VidañosNo ratings yet
- Patogisiologi Dan ChlortalidoneDocument7 pagesPatogisiologi Dan Chlortalidonearya kresnaNo ratings yet
- 33 PDFDocument3 pages33 PDFZeptalanNo ratings yet
- HIE and CVSDocument11 pagesHIE and CVSakshayajainaNo ratings yet
- Stress Mechanisms in HypertensionDocument3 pagesStress Mechanisms in Hypertensionaldy umasangadjiNo ratings yet
- Facts From FloridaDocument9 pagesFacts From FloridafbomxdijzyorNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptMuhammad Dadan KurniawanNo ratings yet
- The Autonomic Nervous System and Cardiovascular Health and DiseaseDocument3 pagesThe Autonomic Nervous System and Cardiovascular Health and DiseaseadeNo ratings yet
- Pathophysiology of HeadacheDocument6 pagesPathophysiology of HeadacheMonica Wyona LorensiaNo ratings yet
- Application of Ultrasound in Pulseless Electrical Activity (PEA) Cardiac ArrestDocument3 pagesApplication of Ultrasound in Pulseless Electrical Activity (PEA) Cardiac ArrestKelvin AKNo ratings yet
- Scratching The Surface of Hypoxic Cerebral Vascular Control: A Potentially Polarizing View of Mechanistic Research in HumansDocument5 pagesScratching The Surface of Hypoxic Cerebral Vascular Control: A Potentially Polarizing View of Mechanistic Research in HumanscutkilerNo ratings yet
- Fisiopatología EstatusDocument14 pagesFisiopatología EstatusDaniel LeivaNo ratings yet
- Narrative Review of Clinical Practice Guidelines.15Document12 pagesNarrative Review of Clinical Practice Guidelines.15abraham rumayaraNo ratings yet
- Effect of Early Mobilization in HerniotomyDocument7 pagesEffect of Early Mobilization in Herniotomyabraham rumayaraNo ratings yet
- Educational Level & QoLDocument7 pagesEducational Level & QoLFerdy LainsamputtyNo ratings yet
- Occupational Stress and Cardiovascular DiseaseDocument8 pagesOccupational Stress and Cardiovascular Diseaseabraham rumayaraNo ratings yet
- Claudia A. S. Araujo (Corresponding Author)Document51 pagesClaudia A. S. Araujo (Corresponding Author)abraham rumayaraNo ratings yet
- Gentamicyn Use To Treat The Wound-In Combination With Other DrugsDocument12 pagesGentamicyn Use To Treat The Wound-In Combination With Other Drugsabraham rumayaraNo ratings yet
- Cir 0000000000000985Document20 pagesCir 0000000000000985abraham rumayaraNo ratings yet
- Why We Need To Know Patients' Education: Invited CommentaryDocument2 pagesWhy We Need To Know Patients' Education: Invited Commentaryabraham rumayaraNo ratings yet
- Why Does Chronic Heart Failure Cause Breathlessness and Fatigue?Document19 pagesWhy Does Chronic Heart Failure Cause Breathlessness and Fatigue?abraham rumayaraNo ratings yet
- Kubota 2017Document8 pagesKubota 2017abraham rumayaraNo ratings yet
- Accepted Manuscript: 10.1016/j.cardfail.2015.09.016Document24 pagesAccepted Manuscript: 10.1016/j.cardfail.2015.09.016abraham rumayaraNo ratings yet
- Ehq 435Document9 pagesEhq 435abraham rumayaraNo ratings yet
- Impact of Patient Education On Chronic Heart Failure in Primary Care (ETIC) : A Cluster Randomised TrialDocument13 pagesImpact of Patient Education On Chronic Heart Failure in Primary Care (ETIC) : A Cluster Randomised Trialabraham rumayaraNo ratings yet
- Impairment of Ventilatory Efficiency in Heart Failure: Prognostic ImpactDocument8 pagesImpairment of Ventilatory Efficiency in Heart Failure: Prognostic Impactabraham rumayaraNo ratings yet
- Borg ScaleDocument6 pagesBorg Scaleabraham rumayaraNo ratings yet
- Symptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree SurvivalDocument10 pagesSymptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree Survivalabraham rumayaraNo ratings yet
- Thank GodDocument6 pagesThank Godabraham rumayaraNo ratings yet
- Why Does Chronic Heart Failure Cause Breathlessness and Fatigue?Document19 pagesWhy Does Chronic Heart Failure Cause Breathlessness and Fatigue?abraham rumayaraNo ratings yet
- Predicting Trends in Dyspnea and Fatigue in Heart Failure Patients' OutcomesDocument8 pagesPredicting Trends in Dyspnea and Fatigue in Heart Failure Patients' Outcomesabraham rumayaraNo ratings yet
- Simple Methods of Assessing Physical Activity in Patients With Chronic Heart FailureDocument6 pagesSimple Methods of Assessing Physical Activity in Patients With Chronic Heart Failureabraham rumayaraNo ratings yet
- New 4Document11 pagesNew 4abraham rumayaraNo ratings yet
- Identification, Associated Factors, and Prognosis of Symptom Clusters in Taiwanese Patients With Heart FailureDocument8 pagesIdentification, Associated Factors, and Prognosis of Symptom Clusters in Taiwanese Patients With Heart Failureabraham rumayaraNo ratings yet
- Sex-Specific Trends in Incidence and Mortality For Urban and Rural Ambulatory Patients With Heart Failure in Eastern Ontario From 1994 To 2013Document7 pagesSex-Specific Trends in Incidence and Mortality For Urban and Rural Ambulatory Patients With Heart Failure in Eastern Ontario From 1994 To 2013abraham rumayaraNo ratings yet
- Sex-Specific Differences in New York Heart Association Classification and Outcomes of Decompensated Heart FailureDocument3 pagesSex-Specific Differences in New York Heart Association Classification and Outcomes of Decompensated Heart Failureabraham rumayaraNo ratings yet
- Temporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million IndividualsDocument9 pagesTemporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million Individualsabraham rumayaraNo ratings yet
- TX GodDocument6 pagesTX Godabraham rumayaraNo ratings yet
- Thank God2Document6 pagesThank God2abraham rumayaraNo ratings yet
- Identification, Associated Factors, and Prognosis of Symptom Clusters in Taiwanese Patients With Heart FailureDocument8 pagesIdentification, Associated Factors, and Prognosis of Symptom Clusters in Taiwanese Patients With Heart Failureabraham rumayaraNo ratings yet
- Gender and Heart Failure: A Population Perspective: P A Mehta, M R CowieDocument5 pagesGender and Heart Failure: A Population Perspective: P A Mehta, M R Cowieabraham rumayaraNo ratings yet
- Comparing and Contrasting Lady Macbeth and Ophelia From HamletDocument5 pagesComparing and Contrasting Lady Macbeth and Ophelia From HamletYashika MalhotraNo ratings yet
- Essential Nutrients - Minerals: 6.1 Introduction and ClassificationDocument15 pagesEssential Nutrients - Minerals: 6.1 Introduction and ClassificationRavinder RanaNo ratings yet
- Infantile Seizure Presentation SlidesDocument7 pagesInfantile Seizure Presentation Slidesjuliana marquezNo ratings yet
- Hyoscine ButylbromideDocument2 pagesHyoscine ButylbromideKenneth ColeNo ratings yet
- Unit 3Document15 pagesUnit 3Neenu RajputNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet
- Vyankatesh City-IIDocument17 pagesVyankatesh City-IIapi-27095887No ratings yet
- Uts Ganjil Bahasa Inggris Kelas 9Document11 pagesUts Ganjil Bahasa Inggris Kelas 9Ketua EE 2021 AndrianoNo ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- Nepal New Emerging Pharma MarketDocument5 pagesNepal New Emerging Pharma MarketDeep_HeartNo ratings yet
- Introducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsDocument24 pagesIntroducing Behavioural Markers of Non-Technical Skills in Oil and Gas OperationsMarutpal MukherjeeNo ratings yet
- Sensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotDocument23 pagesSensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotCaguioa Mark Anthony G.No ratings yet
- Sattvika Dite-YakubDocument6 pagesSattvika Dite-Yakubyakubjacob100% (1)
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
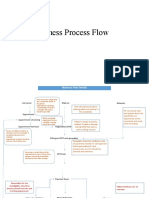
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Myocardial Protection - An UpdateDocument67 pagesMyocardial Protection - An UpdateRezwanul Hoque Bulbul100% (5)
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- Plasma Metanephrine Test: Patient Information FactsheetDocument2 pagesPlasma Metanephrine Test: Patient Information FactsheetDamigart PremiumNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Test Bank For Mosbys Essentials For Nursing Assistants 4th Edition SorrentinoDocument24 pagesTest Bank For Mosbys Essentials For Nursing Assistants 4th Edition Sorrentinozacharymcleanpdqogjyfeb100% (47)
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet