You might also like
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- NOAF en Paciente Critico RevisionDocument11 pagesNOAF en Paciente Critico RevisionARTURO YOSHIMAR LUQUE MAMANINo ratings yet
- J Jacc 2018 05 027Document14 pagesJ Jacc 2018 05 027totya91No ratings yet
- Clinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With HeartDocument13 pagesClinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With Heartrizkiyah prabawantiNo ratings yet
- 10.1016@S0140 67361932317 7Document11 pages10.1016@S0140 67361932317 7DaviSalmissonNo ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO GuidelineDocument17 pagesImmunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers: ASCO GuidelineDrDeepak MittalNo ratings yet
- Jain 2016 Defining The Role of UltrafiltratioDocument9 pagesJain 2016 Defining The Role of UltrafiltratioAbdallah H. KamelNo ratings yet
- 2023 AJTM Vol 7 Issue 1 Article 7Document9 pages2023 AJTM Vol 7 Issue 1 Article 7gzou2013No ratings yet
- 2013 Surgical Prophylaxis ASHP, IDSA, SHEA, SISDocument8 pages2013 Surgical Prophylaxis ASHP, IDSA, SHEA, SISMara Medina - BorleoNo ratings yet
- Packer 2019Document14 pagesPacker 2019Renata D GNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptIntan Kartika NursyahbaniNo ratings yet
- E1512 FullDocument16 pagesE1512 Fullamilkar morunoNo ratings yet
- CVS Toxicity Anticancer Systematic ReviewDocument15 pagesCVS Toxicity Anticancer Systematic ReviewprasanbhandariNo ratings yet
- Nihms 271845Document17 pagesNihms 271845Andres Mauricio MuñozNo ratings yet
- NIH Public Access: Concise Definitive Review: Focused Critical Care Echocardiography in The ICUDocument17 pagesNIH Public Access: Concise Definitive Review: Focused Critical Care Echocardiography in The ICUJelena Obrenovic StankovicNo ratings yet
- 1013 Vasoactive Agents in ShockDocument20 pages1013 Vasoactive Agents in Shockrogelio cruzNo ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- NIH Public Access: Author ManuscriptDocument26 pagesNIH Public Access: Author Manuscriptchrist_cruzerNo ratings yet
- 15.promoting End-Of-Life Discussions in Advanced CancerDocument15 pages15.promoting End-Of-Life Discussions in Advanced Cancerbunga mawarNo ratings yet
- Association Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisDocument7 pagesAssociation Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisbernardoNo ratings yet
- Prognostic Markers Compared To CD3 TIL in Locally.83Document7 pagesPrognostic Markers Compared To CD3 TIL in Locally.83Yohana Elisabeth GultomNo ratings yet
- Artigo 2Document20 pagesArtigo 2ANDREZA ALMEIDANo ratings yet
- NIH Public AccessDocument20 pagesNIH Public Accessaaasim93No ratings yet
- NIH Public AccessDocument13 pagesNIH Public Accessevi munjayantiNo ratings yet
- Exercise and Other Non-Pharmaceutical Interventions 2018Document10 pagesExercise and Other Non-Pharmaceutical Interventions 2018storm.ghirlandoNo ratings yet
- HHS Public Access: Intradialytic Activities and Health-Related Quality of Life Among Hemodialysis PatientsDocument16 pagesHHS Public Access: Intradialytic Activities and Health-Related Quality of Life Among Hemodialysis PatientslamyaaNo ratings yet
- The Benefit of Dysphagia Screening in Adult Patients With Stroke A Meta-AnalysisDocument61 pagesThe Benefit of Dysphagia Screening in Adult Patients With Stroke A Meta-AnalysisAlexandreNo ratings yet
- Clinical Examination in The Heart FaillureDocument9 pagesClinical Examination in The Heart FaillureKaren SerranoNo ratings yet
- Prevencion Del Tev en NeurocirugiaDocument15 pagesPrevencion Del Tev en NeurocirugiaRicardo GarciaNo ratings yet
- Jamaoncology Reyngold 2021 BR 210002 1621005075.20653Document4 pagesJamaoncology Reyngold 2021 BR 210002 1621005075.20653Gloribel BolívarNo ratings yet
- Ricardo - Management of Lung Nodules and Lung Cancer Screening During COVIDDocument10 pagesRicardo - Management of Lung Nodules and Lung Cancer Screening During COVIDCIRUGIA CARDIOTORÁCICA MINIMAMENTE INVASIVANo ratings yet
- Physycal Examination On CV SystemDocument21 pagesPhysycal Examination On CV SystemMerellyn Hurtado PachecoNo ratings yet
- Ijbs 24374Document8 pagesIjbs 24374Putri Tamara DasantosNo ratings yet
- American Thoracic Society DocumentsDocument10 pagesAmerican Thoracic Society DocumentsEviNo ratings yet
- Circulationaha 121 054990Document32 pagesCirculationaha 121 054990mrabhilekhNo ratings yet
- Predicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentDocument14 pagesPredicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentRoberto López MataNo ratings yet
- Guideline VaskularDocument251 pagesGuideline VaskularjeannchristyNo ratings yet
- EchoMonitor2015 PDFDocument17 pagesEchoMonitor2015 PDFmarkleacockNo ratings yet
- Hirsch Et Al 2023 Critical Care Management of Patients After Cardiac Arrest A Scientific Statement From The AmericanDocument33 pagesHirsch Et Al 2023 Critical Care Management of Patients After Cardiac Arrest A Scientific Statement From The AmericanHelder LezamaNo ratings yet
- 2008-Predictive Validity of A Medication Adherence Measure in An Outpatient Setting PDFDocument7 pages2008-Predictive Validity of A Medication Adherence Measure in An Outpatient Setting PDFRizki RomadhonNo ratings yet
- Ni Hms 537812Document15 pagesNi Hms 537812maracioNo ratings yet
- SSC Guidelines 2012Document64 pagesSSC Guidelines 2012David GonNo ratings yet
- Kdoqi PDFDocument164 pagesKdoqi PDFcindyrelyNo ratings yet
- Blumenthal Et Al 2018 Patient Reported Outcomes in CardiologyDocument4 pagesBlumenthal Et Al 2018 Patient Reported Outcomes in CardiologyMariana SantosNo ratings yet
- Ultrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015Document10 pagesUltrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015angelama1783riosNo ratings yet
- Effectiveness of Pressure Ulcer Prevention Strategies For Adult Patients in Intensive Care Units: A Systematic ReviewDocument13 pagesEffectiveness of Pressure Ulcer Prevention Strategies For Adult Patients in Intensive Care Units: A Systematic ReviewKayam SinghNo ratings yet
- Electrocardiographic Monitoring 2017Document72 pagesElectrocardiographic Monitoring 2017Mirela Marina BlajNo ratings yet
- Aritmia - SRMA Akup Dan HerbalDocument8 pagesAritmia - SRMA Akup Dan HerbalJacquelyn KellyNo ratings yet
- Vestibular CPG JNPT 2016 FinalDocument33 pagesVestibular CPG JNPT 2016 FinalMairaNo ratings yet
- BallDocument8 pagesBallAllan Alejandro SevillaNo ratings yet
- RCP y PH ArterialDocument2 pagesRCP y PH ArterialPaola LizarzabalNo ratings yet
- Evidence-Based Drug Therapy For Chronic Heart Failure: ZannadDocument7 pagesEvidence-Based Drug Therapy For Chronic Heart Failure: ZannadA5BNi Gusti Ketut Purnami Putri AdnyaniNo ratings yet
- Subutilizacion de ACO en Adultos Mayores en EEUU-2022Document12 pagesSubutilizacion de ACO en Adultos Mayores en EEUU-2022Walter ReyesNo ratings yet
- Preoperative Evaluation in The 21st CenturyDocument13 pagesPreoperative Evaluation in The 21st CenturyPaulHerrera0% (1)
- Diagnosis and Evaluation of Hypersensitivity Pneumonitis: CHEST Guideline and Expert Panel ReportDocument60 pagesDiagnosis and Evaluation of Hypersensitivity Pneumonitis: CHEST Guideline and Expert Panel Reportjose henaoNo ratings yet
- 793 FullDocument9 pages793 FullDENNYNo ratings yet
- PAH Survival 2010Document28 pagesPAH Survival 2010Mikhael AsafNo ratings yet
- Clinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyDocument8 pagesClinical Guideline Diagnosing Syncope Part 1: Value of History, Physical Examination, and ElectrocardiographyPriya JainNo ratings yet
- Effect of Early Mobilization in HerniotomyDocument7 pagesEffect of Early Mobilization in Herniotomyabraham rumayaraNo ratings yet
- Narrative Review of Clinical Practice Guidelines.15Document12 pagesNarrative Review of Clinical Practice Guidelines.15abraham rumayaraNo ratings yet
- Why We Need To Know Patients' Education: Invited CommentaryDocument2 pagesWhy We Need To Know Patients' Education: Invited Commentaryabraham rumayaraNo ratings yet
- Ehq 435Document9 pagesEhq 435abraham rumayaraNo ratings yet
- Cir 0000000000000985Document20 pagesCir 0000000000000985abraham rumayaraNo ratings yet
- Borg ScaleDocument6 pagesBorg Scaleabraham rumayaraNo ratings yet
- TX GodDocument6 pagesTX Godabraham rumayaraNo ratings yet
- Impairment of Ventilatory Efficiency in Heart Failure: Prognostic ImpactDocument8 pagesImpairment of Ventilatory Efficiency in Heart Failure: Prognostic Impactabraham rumayaraNo ratings yet
- Kubota 2017Document8 pagesKubota 2017abraham rumayaraNo ratings yet
- Accepted Manuscript: 10.1016/j.cardfail.2015.09.016Document24 pagesAccepted Manuscript: 10.1016/j.cardfail.2015.09.016abraham rumayaraNo ratings yet
- Simple Methods of Assessing Physical Activity in Patients With Chronic Heart FailureDocument6 pagesSimple Methods of Assessing Physical Activity in Patients With Chronic Heart Failureabraham rumayaraNo ratings yet
- Oxen Ham 2003Document9 pagesOxen Ham 2003abraham rumayaraNo ratings yet
- Why Does Chronic Heart Failure Cause Breathlessness and Fatigue?Document19 pagesWhy Does Chronic Heart Failure Cause Breathlessness and Fatigue?abraham rumayaraNo ratings yet
- Symptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree SurvivalDocument10 pagesSymptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree Survivalabraham rumayaraNo ratings yet
- Predicting Trends in Dyspnea and Fatigue in Heart Failure Patients' OutcomesDocument8 pagesPredicting Trends in Dyspnea and Fatigue in Heart Failure Patients' Outcomesabraham rumayaraNo ratings yet
- New 4Document11 pagesNew 4abraham rumayaraNo ratings yet
- Gender and Heart Failure: A Population Perspective: P A Mehta, M R CowieDocument5 pagesGender and Heart Failure: A Population Perspective: P A Mehta, M R Cowieabraham rumayaraNo ratings yet
- Sex-Specific Trends in Incidence and Mortality For Urban and Rural Ambulatory Patients With Heart Failure in Eastern Ontario From 1994 To 2013Document7 pagesSex-Specific Trends in Incidence and Mortality For Urban and Rural Ambulatory Patients With Heart Failure in Eastern Ontario From 1994 To 2013abraham rumayaraNo ratings yet
- Thank GodDocument6 pagesThank Godabraham rumayaraNo ratings yet
- Strait 2012Document22 pagesStrait 2012abraham rumayaraNo ratings yet
- TX GodDocument6 pagesTX Godabraham rumayaraNo ratings yet
- Temporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million IndividualsDocument9 pagesTemporal Trends and Patterns in Heart Failure Incidence: A Population-Based Study of 4 Million Individualsabraham rumayaraNo ratings yet
- Pen TingDocument9 pagesPen Tingabraham rumayaraNo ratings yet
- Antihypertensive DrugsDocument2 pagesAntihypertensive Drugsbalyaibnu_690869145100% (1)
- MSG83 Epidural Analgesia in Labour PDFDocument18 pagesMSG83 Epidural Analgesia in Labour PDFGrigore PopaNo ratings yet
- A Detailed Plan in ScienceDocument5 pagesA Detailed Plan in ScienceAmpolitozNo ratings yet
- Cardiac EmergenciesDocument73 pagesCardiac EmergenciesKristine CaringalNo ratings yet
- The Cardiovascular System - WorksheetDocument6 pagesThe Cardiovascular System - WorksheetLe Thi Huong TraNo ratings yet
- Adrenergic Antagonist (2013)Document23 pagesAdrenergic Antagonist (2013)Akmal SafwanNo ratings yet
- Neonatal Asphyxia PDFDocument10 pagesNeonatal Asphyxia PDFrhimezNo ratings yet
- Fracture Nursing Care PlansDocument14 pagesFracture Nursing Care PlansSheryl Ann Barit PedinesNo ratings yet
- RenalDocument25 pagesRenalCamaligan RockyNo ratings yet
- Liver Diseases in PregnancyDocument5 pagesLiver Diseases in PregnancyOana TimofteNo ratings yet
- NIH Document Production Cover Letter 2021.10.20 McMorris RodgersDocument2 pagesNIH Document Production Cover Letter 2021.10.20 McMorris RodgersAl StatiliusNo ratings yet
- Congenital and Hereditary Diseases Introduction-1Document21 pagesCongenital and Hereditary Diseases Introduction-1Melvin OnyanchaNo ratings yet
- re-FINAL REPORT ON BLOOD DONATIONDocument31 pagesre-FINAL REPORT ON BLOOD DONATIONPreeti ChouhanNo ratings yet
- MODULE 4 - Fil AkadDocument3 pagesMODULE 4 - Fil Akademilia asunaNo ratings yet
- PathfitDocument3 pagesPathfitKaren CastorNo ratings yet
- Annotated BibDocument19 pagesAnnotated Bibapi-252208553No ratings yet
- Vice and Drugs Education Reviewer - 070753Document16 pagesVice and Drugs Education Reviewer - 070753alliahshane.borromeoNo ratings yet
- Journal Reading AminophyllineDocument76 pagesJournal Reading AminophyllinePandhu Suprobo100% (1)
- Abdominal TraumaDocument60 pagesAbdominal Traumaapi-19916399No ratings yet
- DR Craig WeilDocument14 pagesDR Craig WeilPaula OwensNo ratings yet
- Dinesh RamDocument1 pageDinesh RamchandanNo ratings yet
- Congenital and Development Anomalies of The KidneyDocument4 pagesCongenital and Development Anomalies of The KidneyEMILY N CRUZ-VARGASNo ratings yet
- Tugas MakalahDocument4 pagesTugas MakalahPita AnggraeniNo ratings yet
- Substance Abuse Handout MCHDocument5 pagesSubstance Abuse Handout MCHfdgrgNo ratings yet
- Antemortem and Post Mortem InspectionDocument15 pagesAntemortem and Post Mortem InspectionMuhammad SiddiqueNo ratings yet
- Liver Function TestDocument89 pagesLiver Function Testprashanthsham100% (1)
- Lecture Planner - Zoology - (Only PDFDocument1 pageLecture Planner - Zoology - (Only PDFsatyamkeshari90807060No ratings yet
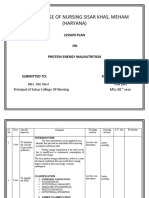
- Lesson Plan On PemDocument19 pagesLesson Plan On Pemanil jain0% (1)
- Virus Hepatitis RevDocument83 pagesVirus Hepatitis RevSukma WinahyuNo ratings yet
- Rough Draft of Our Case Pre..14 NovDocument41 pagesRough Draft of Our Case Pre..14 NovJhoyee MangyaoNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (41)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (171)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (4)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)