You might also like
- The Shutdown Dissociation Scale (Shut-D)Document13 pagesThe Shutdown Dissociation Scale (Shut-D)Helena QuintNo ratings yet
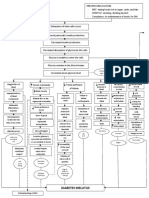
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Buteyko Manual PDFDocument130 pagesButeyko Manual PDFPauloCarvalho92% (12)
- The Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Document348 pagesThe Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Andreea0% (1)
- Laboratory Diagnosis of Infectious Diseases GuidelineDocument100 pagesLaboratory Diagnosis of Infectious Diseases GuidelineGalo PinosNo ratings yet
- Maxwell's Manual of Malicious MaladiesDocument35 pagesMaxwell's Manual of Malicious MaladiesJean Ariehn100% (1)
- International Days CalendarDocument6 pagesInternational Days CalendarCorkChoral0% (1)
- The para My Xo VirusesDocument608 pagesThe para My Xo VirusesJOAO ZOLINI GOMESNo ratings yet
- Jurnal TBCDocument6 pagesJurnal TBCLorinsya Ollin100% (1)
- COVID-19 AWARENESS PPT FinalDocument37 pagesCOVID-19 AWARENESS PPT FinalFranz goNo ratings yet
- MONKEYPOX Artigo Primeiro Caso Monkeypox Brasil RIMTSPDocument4 pagesMONKEYPOX Artigo Primeiro Caso Monkeypox Brasil RIMTSPthaistoledofinkNo ratings yet
- Identifying Paracoccidioides Phylogenetic Species by PCR-RFLP of The Alpha-Tubulin GeneDocument8 pagesIdentifying Paracoccidioides Phylogenetic Species by PCR-RFLP of The Alpha-Tubulin GeneKirana agist wangsa putriNo ratings yet
- SARS-CoV-2 and Arbovirus Infection - A Rapid Systematic Review PDFDocument7 pagesSARS-CoV-2 and Arbovirus Infection - A Rapid Systematic Review PDFNelson Carvas JrNo ratings yet
- Poster Abstracts - OFID 2019:6 (Suppl 2) - S297Document1 pagePoster Abstracts - OFID 2019:6 (Suppl 2) - S297ELIONo ratings yet
- Journal Pre-Proof: Vacunas: Investigaci On y PR ActicaDocument12 pagesJournal Pre-Proof: Vacunas: Investigaci On y PR ActicaMohammed Shuaib AhmedNo ratings yet
- PIIS0195670124000720Document19 pagesPIIS0195670124000720Jorge MirandaNo ratings yet
- Pseudomonas 2024Document39 pagesPseudomonas 2024Yorvi hendersson Ilasaca gaonaNo ratings yet
- Jurnal 2Document10 pagesJurnal 2GFORCE .ID.No ratings yet
- International Journal of Microbiology Research: January 2013Document7 pagesInternational Journal of Microbiology Research: January 2013DDRNo ratings yet
- Miotto. Interpreting Mutations and Phenotypic DR. ERJ 2019Document13 pagesMiotto. Interpreting Mutations and Phenotypic DR. ERJ 2019Vigilancia EpidemiologicaNo ratings yet
- G. Leite. Genes Differentially Expressed by TB After Exposure To Ruthenium Phosphinic Compound and IsoniazidDocument6 pagesG. Leite. Genes Differentially Expressed by TB After Exposure To Ruthenium Phosphinic Compound and IsoniazidBrayan CamposNo ratings yet
- 20 01 PDFDocument26 pages20 01 PDFT h o r y n R a m o sNo ratings yet
- 2018 Recommendations For The Management of Community Acquired PnemoniaDocument19 pages2018 Recommendations For The Management of Community Acquired PnemoniaMonica ReyesNo ratings yet
- Candida MicDocument5 pagesCandida MicKalpanaNo ratings yet
- (IJCST-V4I4P22) : Elena Trajkovska-Dokic, Snezana Stojkovska, Milena Petrovska, Nikola PanovskiDocument4 pages(IJCST-V4I4P22) : Elena Trajkovska-Dokic, Snezana Stojkovska, Milena Petrovska, Nikola PanovskiEighthSenseGroupNo ratings yet
- Procalcitonin, C-Reactive Protein, Albumin, and Blood Cultures As Early Markers of Sepsis Diagnosis or Predictors of Outcome: A Prospective AnalysisDocument7 pagesProcalcitonin, C-Reactive Protein, Albumin, and Blood Cultures As Early Markers of Sepsis Diagnosis or Predictors of Outcome: A Prospective Analysistaufik.abdiNo ratings yet
- Synthesis and Anti-Chikungunya Virus (CHIKV) Activity of Novel 2022Document14 pagesSynthesis and Anti-Chikungunya Virus (CHIKV) Activity of Novel 2022Daniel Tadeu Gomes GonzagaNo ratings yet
- 1 s2.0 S0753332223007874 MainDocument18 pages1 s2.0 S0753332223007874 MainFernando del BlancoNo ratings yet
- Thesis Paper On PneumoniaDocument7 pagesThesis Paper On Pneumoniagbwwdfq5100% (1)
- VanDevanter 2019Document23 pagesVanDevanter 2019Aya AlkhatibNo ratings yet
- Bmri2016 8905675Document9 pagesBmri2016 8905675helderjamsNo ratings yet
- Gamberini Et AlDocument9 pagesGamberini Et AlDeboraXiningNo ratings yet
- EMI Conspiracy ZlshiDocument10 pagesEMI Conspiracy ZlshiOstflopNo ratings yet
- Immunodiagnosis of Paracoccidioidomycosis Due To Paracoccidioides Brasiliensis Using A Latex Test: Detection of Specifi...Document17 pagesImmunodiagnosis of Paracoccidioidomycosis Due To Paracoccidioides Brasiliensis Using A Latex Test: Detection of Specifi...PinkiPonki2No ratings yet
- Christiansen 2014 ISHCIDocument8 pagesChristiansen 2014 ISHCICerlyn CabanitNo ratings yet
- Oxford University Press Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Clinical Infectious DiseasesDocument13 pagesOxford University Press Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Clinical Infectious DiseasesPisi MicaNo ratings yet
- Medicina 57 00852Document4 pagesMedicina 57 00852PhDmónica Rios SilvaNo ratings yet
- Identification of Bacterial Plant Pathogens Using Multilocus Polymerase Chain Reaction/Electrospray Ionization-Mass SpectrometryDocument9 pagesIdentification of Bacterial Plant Pathogens Using Multilocus Polymerase Chain Reaction/Electrospray Ionization-Mass SpectrometryEdwin Josua SilabanNo ratings yet
- And Evaluation of PCR For Diagnosis Of: Bordetella Parapertussis Pertussis BordetellaDocument6 pagesAnd Evaluation of PCR For Diagnosis Of: Bordetella Parapertussis Pertussis BordetellaAsri RachmawatiNo ratings yet
- Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesDocument4 pagesPredicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic SamplesArum Rahmawatie VirgieNo ratings yet
- Plasmid-Mediated Transmission of KPC-2 Carbapenema PDFDocument8 pagesPlasmid-Mediated Transmission of KPC-2 Carbapenema PDFJose Daniel Muñoz FuentesNo ratings yet
- Makalah Biologi MolekulerDocument11 pagesMakalah Biologi MolekulerSarah PanjaitanNo ratings yet
- KCP 1Document7 pagesKCP 1FurqanRidhaNo ratings yet
- 2019 - Pan Proteome of Xanthomonas Campestris Pv. CampestrisDocument10 pages2019 - Pan Proteome of Xanthomonas Campestris Pv. CampestrisMariana Rocha MaximianoNo ratings yet
- Preprint Not Peer Reviewed: STOBE: A Long-COVID Syndromic Study Using Real-World Data in BrazilDocument35 pagesPreprint Not Peer Reviewed: STOBE: A Long-COVID Syndromic Study Using Real-World Data in BrazilDr. Heitor Cavalini FisioterapeutaNo ratings yet
- Journal Pre-Proof: New Microbes and New InfectionsDocument16 pagesJournal Pre-Proof: New Microbes and New InfectionsLalram Zaua Marama100% (1)
- Villagomez 2021Document1 pageVillagomez 2021DANIEL ARTEAGA MENDOZANo ratings yet
- SSRN Id3902468Document20 pagesSSRN Id3902468JaimeNo ratings yet
- Ebook Advances in Parasitology Volume 117 PDF Full Chapter PDFDocument67 pagesEbook Advances in Parasitology Volume 117 PDF Full Chapter PDFnan.huelse294100% (30)
- CDC 30614 DS1Document29 pagesCDC 30614 DS1David Sergio Salas VargasNo ratings yet
- MLB 110 - MLS - E - 1920 - 02 B (1) (1) ExamsDocument6 pagesMLB 110 - MLS - E - 1920 - 02 B (1) (1) Examsmaxwell amponsahNo ratings yet
- Boursiani 2017Document5 pagesBoursiani 2017Carlos Urkieta MonetaNo ratings yet
- (Advances in Parasitology 50) - Academic Press (2001)Document275 pages(Advances in Parasitology 50) - Academic Press (2001)Stoian GoranovNo ratings yet
- Journal Pre-Proof: Clinical Microbiology and InfectionDocument24 pagesJournal Pre-Proof: Clinical Microbiology and InfectionFrancisco BettencourtNo ratings yet
- Efficacy of Proxalutamide in Hospitalized COVID-19 .FullDocument45 pagesEfficacy of Proxalutamide in Hospitalized COVID-19 .FullGerte Donti FantiaNo ratings yet
- The Diagnostic Value of Neutrophil CD64 in Detection of Sepsis in ChildrenDocument5 pagesThe Diagnostic Value of Neutrophil CD64 in Detection of Sepsis in ChildrenrinaviviaudianaNo ratings yet
- Jurnal CT ValueDocument3 pagesJurnal CT ValueMetha AgustinaNo ratings yet
- 2020 12 21 20248640v1 FullDocument19 pages2020 12 21 20248640v1 Fulla sangNo ratings yet
- Immunology Letters: SciencedirectDocument6 pagesImmunology Letters: SciencedirectLaila Kurnia PramonoNo ratings yet
- Evaluation of Enzyme Producing K. Pneumoniae and Their Susceptibility To Other Anti-BioticsDocument3 pagesEvaluation of Enzyme Producing K. Pneumoniae and Their Susceptibility To Other Anti-BioticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Informe: Laboratorio de Genética para Microbiología, Martes-1500Document52 pagesInforme: Laboratorio de Genética para Microbiología, Martes-1500GenesisNo ratings yet
- 2015 Monitoringofthe Parasite LoadDocument24 pages2015 Monitoringofthe Parasite LoadMarcio FonteneleNo ratings yet
- Analytical Performance of COVID-19 Detection Methods (RT-PCR) : Scientific and Societal ConcernsDocument16 pagesAnalytical Performance of COVID-19 Detection Methods (RT-PCR) : Scientific and Societal ConcernsFre mobileNo ratings yet
- Programa Final SBCCH 2015edDocument40 pagesPrograma Final SBCCH 2015edNicolás Martínez AlarcónNo ratings yet
- Chapter E132 - Coronavirus Disease (COVID-19)Document31 pagesChapter E132 - Coronavirus Disease (COVID-19)AnasM.GhannoumNo ratings yet
- The Radiation Boom - As Technology Surges, Radiation Safeguards Lag - Series - NYTimesDocument12 pagesThe Radiation Boom - As Technology Surges, Radiation Safeguards Lag - Series - NYTimesMuh Taufik Dwi PutraNo ratings yet
- 1-3 Day 1 - Community As People Community Health NursingDocument11 pages1-3 Day 1 - Community As People Community Health NursingBea Dela CenaNo ratings yet
- Hematology India: QuestionsDocument22 pagesHematology India: QuestionsSelim TarekNo ratings yet
- Coping With Diabetes-Denial, AngerDocument13 pagesCoping With Diabetes-Denial, AngerShwetal ShindeNo ratings yet
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet
- Diabetes InsipidusDocument1 pageDiabetes InsipidusAnold ShangaliNo ratings yet
- Table of Contents - ChestDocument7 pagesTable of Contents - ChestKaran KalraNo ratings yet
- Fit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full ChapterDocument41 pagesFit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full Chapterwilliam.decker273100% (26)
- A Comparative Clinical Study On The Effect of Mrittika Lepa and Lodhradi Lepa in Yuvanapidika W.S.R To Acne VulgarisDocument6 pagesA Comparative Clinical Study On The Effect of Mrittika Lepa and Lodhradi Lepa in Yuvanapidika W.S.R To Acne VulgarisIJAR JOURNALNo ratings yet
- Ozone Therapy A New Exemplar in DentistryDocument5 pagesOzone Therapy A New Exemplar in DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pelvic Inflammatory Disease-SCIENCEDocument7 pagesPelvic Inflammatory Disease-SCIENCELeanne Marie Paredes TanNo ratings yet
- Managing Safety and HealthDocument40 pagesManaging Safety and HealthFairooz RaisaNo ratings yet
- np4 TestDocument8 pagesnp4 TestMargie BalunesNo ratings yet
- Case Study AnalysisDocument3 pagesCase Study AnalysisDominique LopenaNo ratings yet
- dotAIO V2 LiteDocument1 pagedotAIO V2 LiteStevanusNo ratings yet
- Module 14Document9 pagesModule 14mirai desuNo ratings yet
- GREENLEAFDocument5 pagesGREENLEAF-Cabinet de traduction NETWORDTNo ratings yet
- Emergency NursingDocument5 pagesEmergency NursingRomeoJunoNo ratings yet
- Anestesia de Animales ExoticosDocument13 pagesAnestesia de Animales ExoticosDIANA MABEL PAGUAY CAJASNo ratings yet
- Aneurisma de La Arteria HumeralDocument3 pagesAneurisma de La Arteria HumeralcastillojessNo ratings yet
- Rehabilitasi AGA AGBDocument47 pagesRehabilitasi AGA AGBdeasyNo ratings yet
- OMS 190807 - Prequalified - Product - ListDocument11 pagesOMS 190807 - Prequalified - Product - ListYeisy Yainira Leon Gomez100% (1)