You might also like
- List of Registered Non Govt and Govt Secondary SchoolDocument200 pagesList of Registered Non Govt and Govt Secondary SchoolDennisEudes78% (9)
- Daudon CVDocument2 pagesDaudon CVmariusNo ratings yet
- Kidney Stones Pathophysiology, Diagnosis and ManagementDocument13 pagesKidney Stones Pathophysiology, Diagnosis and ManagementNani AlituNo ratings yet
- Climate Bogeyman3 PDFDocument199 pagesClimate Bogeyman3 PDFIonel Leon100% (1)
- Merger Case AnalysisDocument71 pagesMerger Case Analysissrizvi2000No ratings yet
- U S A 1,000 P S T: Rinary Tone Nalysis of Atients IN Outhern AiwanDocument4 pagesU S A 1,000 P S T: Rinary Tone Nalysis of Atients IN Outhern AiwanTanveerNo ratings yet
- Jeremiah Mathura PHYS 3153 FINAL YEAR PROJECT - CRYSTALLOGRAPHIC STUDIES ON KIDNEY STONES 816020063 740749 383137969Document60 pagesJeremiah Mathura PHYS 3153 FINAL YEAR PROJECT - CRYSTALLOGRAPHIC STUDIES ON KIDNEY STONES 816020063 740749 383137969Jeremiah MathuraNo ratings yet
- MuhdetalDocument5 pagesMuhdetalvohneNo ratings yet
- THE Composition OF Urinary Stones IN Central Sindh: Original ArticleDocument5 pagesTHE Composition OF Urinary Stones IN Central Sindh: Original ArticleShaheryar HasanNo ratings yet
- Research Article A Specific Urinary Amino Acid Profile Characterizes People With Kidney StonesDocument7 pagesResearch Article A Specific Urinary Amino Acid Profile Characterizes People With Kidney StonesNandy SwariNo ratings yet
- Urolithiasis - Metabolic Considerations: Case 1Document2 pagesUrolithiasis - Metabolic Considerations: Case 1HardiTariqHammaNo ratings yet
- Predictive Value of Kidney Stone Composition in The Detection of Metabolic AbnormalitiesDocument7 pagesPredictive Value of Kidney Stone Composition in The Detection of Metabolic Abnormalitiesjarivera1300No ratings yet
- Kidney Stone Composition Analysis Using Synchrotron X-Ray DiffractionDocument4 pagesKidney Stone Composition Analysis Using Synchrotron X-Ray DiffractionAD17No ratings yet
- Clinical Study of Urolithiasis Management in Rural HospitalDocument11 pagesClinical Study of Urolithiasis Management in Rural HospitalLusi RustinaNo ratings yet
- IJAPB PAPERDocument25 pagesIJAPB PAPERDurga MadhuriNo ratings yet
- Review Article: Kidney Stone Disease: An Update On Current ConceptsDocument12 pagesReview Article: Kidney Stone Disease: An Update On Current Conceptsrahmat syahiliNo ratings yet
- Concentration Effect of Trace Metals in Jordanian Patients of Urinary CalculiDocument10 pagesConcentration Effect of Trace Metals in Jordanian Patients of Urinary Calculiapi-3803483No ratings yet
- Surgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesDocument10 pagesSurgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pathophysiology-Based Treatment of UrolithiasisDocument7 pagesPathophysiology-Based Treatment of UrolithiasisLea Bali Ulina SinurayaNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet
- 1 s2.0 S2161831323002715 MainDocument15 pages1 s2.0 S2161831323002715 MainAdiyanto DidietNo ratings yet
- Molecular mechanisms of Selaginella lepidophylla chloroform extract's protective effect in lithiasic ratsDocument11 pagesMolecular mechanisms of Selaginella lepidophylla chloroform extract's protective effect in lithiasic ratsPlacido Rojas FrancoNo ratings yet
- A Review On Urolithiasis in Dogs and Cats: Bulgarian Journal of Veterinary MedicineDocument18 pagesA Review On Urolithiasis in Dogs and Cats: Bulgarian Journal of Veterinary MedicinetattaNo ratings yet
- Dien Hoa-Sensor 2020Document15 pagesDien Hoa-Sensor 2020Kim ThắmNo ratings yet
- Adsorption On Apatitic Calcium Phosphates For Drug Delivery: Interaction With Bisphosphonate MoleculesDocument9 pagesAdsorption On Apatitic Calcium Phosphates For Drug Delivery: Interaction With Bisphosphonate MoleculesOumaima BenNo ratings yet
- Nephrolithiasis: Causes, Composition, and PathogenesisDocument34 pagesNephrolithiasis: Causes, Composition, and PathogenesisRadix Eko SetiawanNo ratings yet
- Chemical Analysis of Stones and Its Significance in UrolithiasisDocument8 pagesChemical Analysis of Stones and Its Significance in UrolithiasisNithya sudevNo ratings yet
- Osmoregulasi 2Document14 pagesOsmoregulasi 2Nova Rahma DhiyantiNo ratings yet
- Root Cementum Part 15Document10 pagesRoot Cementum Part 15Sumedha MalshetwarNo ratings yet
- Medical Management of Renal Stone: Review ArticleDocument4 pagesMedical Management of Renal Stone: Review ArticlenaveenNo ratings yet
- SC 20141Document3 pagesSC 20141RelviGuzmanApazaNo ratings yet
- Calcium Oxalate Nephrolithiasis: An Easy Way To Detect An Imbalance Between Promoting and Inhibiting FactorsDocument7 pagesCalcium Oxalate Nephrolithiasis: An Easy Way To Detect An Imbalance Between Promoting and Inhibiting FactorsJames TerryNo ratings yet
- Kidney Stone Disease - An Update On Current Concepts - PMCDocument23 pagesKidney Stone Disease - An Update On Current Concepts - PMCRonNo ratings yet
- Corticotomy AssisstedDocument12 pagesCorticotomy AssisstedRohini TondaNo ratings yet
- Thesis Einddocument Sanne LeveringcopPDFDocument42 pagesThesis Einddocument Sanne LeveringcopPDFMartin WiniarskiNo ratings yet
- Metabolic Evaluation and Recurrence Prevention For Urinary Stone Patients: EAU GuidelinesDocument14 pagesMetabolic Evaluation and Recurrence Prevention For Urinary Stone Patients: EAU Guidelinesapoorva jainNo ratings yet
- Journal Pre-Proof: Forensic Science InternationalDocument21 pagesJournal Pre-Proof: Forensic Science InternationalMatheus PereiraNo ratings yet
- Omcl2015 813737Document7 pagesOmcl2015 813737fadimeatesNo ratings yet
- Validation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONDocument6 pagesValidation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONMARIANNE CASTILLO ESCOBARNo ratings yet
- Cejph - Cjp-Faktor Penyebab UrolithiasisDocument6 pagesCejph - Cjp-Faktor Penyebab UrolithiasisCDKadrianNo ratings yet
- Review Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentDocument9 pagesReview Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentZulfikar BasriNo ratings yet
- Lindenschmidt 1991Document8 pagesLindenschmidt 1991aparna.cNo ratings yet
- 4NQO-Induced Rat Tongue Carcinoma: An Ultrastructural StudyDocument8 pages4NQO-Induced Rat Tongue Carcinoma: An Ultrastructural StudyGlauce L TrevisanNo ratings yet
- Management of Staghorn Renal StonesDocument6 pagesManagement of Staghorn Renal StonesSaratGogoiNo ratings yet
- Lead PoisoningDocument3 pagesLead PoisoningSign UpNo ratings yet
- 4755 ID Hubungan Kandungan Mineral Calcium Magnesium Mangaan Dalam Sumber Air Dengan KejDocument6 pages4755 ID Hubungan Kandungan Mineral Calcium Magnesium Mangaan Dalam Sumber Air Dengan KejJuni rahayuNo ratings yet
- Uji KualitatifDocument6 pagesUji KualitatifJuni rahayuNo ratings yet
- Delivery of Huge Bladder Stone in A Thirty-Five-Year-Old ManDocument3 pagesDelivery of Huge Bladder Stone in A Thirty-Five-Year-Old ManJetsinNo ratings yet
- IJVM - Volume 12 - Issue 4 - Pages 293-303Document11 pagesIJVM - Volume 12 - Issue 4 - Pages 293-303Violet Pet ClinicNo ratings yet
- Kuhn 2356Document11 pagesKuhn 2356Bigotboy SoeNo ratings yet
- Developmental Toxicity of Fe3O4 Nanoparticles On Cysts and Three Larval Stages of Artemia SalinDocument9 pagesDevelopmental Toxicity of Fe3O4 Nanoparticles On Cysts and Three Larval Stages of Artemia SalinKishore GiriNo ratings yet
- Kluwer, 2012Document8 pagesKluwer, 2012hakimNo ratings yet
- 2010 MFR - 61 - 1109 1122 EcologyDocument15 pages2010 MFR - 61 - 1109 1122 EcologySixto Gutiérrez SaavedraNo ratings yet
- Phyllanthus Niruri As A Promising Alternative Treatment For NephrolithiasisDocument8 pagesPhyllanthus Niruri As A Promising Alternative Treatment For NephrolithiasisIndra PradanaNo ratings yet
- Ecotoxicology and Environmental Safety: SciencedirectDocument12 pagesEcotoxicology and Environmental Safety: SciencedirectBella Kusuma DewiNo ratings yet
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDocument3 pagesFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiNo ratings yet
- Development and Optimisation of A Standard Method For Extraction of Microplastics in Mussels by Enzyme Digestion of Soft TissuesDocument21 pagesDevelopment and Optimisation of A Standard Method For Extraction of Microplastics in Mussels by Enzyme Digestion of Soft Tissuessindy gemaeka putriNo ratings yet
- a122010-0062021Document12 pagesa122010-0062021April RahmawatiNo ratings yet
- Drug-induced kidney stones: pathophysiology, prevention and treatmentDocument39 pagesDrug-induced kidney stones: pathophysiology, prevention and treatmentCecep Darwis MuttaqinNo ratings yet
- Mulla Principles of Mohammedan LawDocument13 pagesMulla Principles of Mohammedan LawDaiwik pratap singhNo ratings yet
- Prevalence of Kidney Stones and Their Chemical CompositionsDocument3 pagesPrevalence of Kidney Stones and Their Chemical CompositionsAnjan khadkaNo ratings yet
- 3D Aspects of Kidney Structure and Angioarchitecture in Adult and Aged RatsDocument7 pages3D Aspects of Kidney Structure and Angioarchitecture in Adult and Aged RatsCLPHtheoryNo ratings yet
- Answer EnglishDocument16 pagesAnswer EnglishIsa Silva LeónNo ratings yet
- Spectrochimica Acta Part A: Molecular and Biomolecular SpectrosDocument6 pagesSpectrochimica Acta Part A: Molecular and Biomolecular SpectrosIsa Silva LeónNo ratings yet
- Laboratory-Induced Endolithic Growth in Calcarenites: Biodeteriorating Potential AssessmentDocument14 pagesLaboratory-Induced Endolithic Growth in Calcarenites: Biodeteriorating Potential AssessmentIsa Silva LeónNo ratings yet
- Aerosol Composition and Source Apportionment in The Mexico CityDocument10 pagesAerosol Composition and Source Apportionment in The Mexico CityIsa Silva LeónNo ratings yet
- Redox ChemistryDocument25 pagesRedox ChemistrySantosh G PattanadNo ratings yet
- Islamic Finance AsiaDocument2 pagesIslamic Finance AsiaAhmad FaresNo ratings yet
- 1868 Sop Work at HeightDocument10 pages1868 Sop Work at HeightAbid AzizNo ratings yet
- Surveying 2 Practical 3Document15 pagesSurveying 2 Practical 3Huzefa AliNo ratings yet
- Emotion-WPS OfficeDocument2 pagesEmotion-WPS OfficemikaNo ratings yet
- Learning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eDocument21 pagesLearning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eJp AlvarezNo ratings yet
- Coleção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuDocument1 pageColeção Bernoulli Ensino Médio 2020 - 100% BNCC by Bernoulli Sistema de Ensino - IssuuVitor OliveiraNo ratings yet
- GES1003 AY1819 CLS Tutorial 1Document4 pagesGES1003 AY1819 CLS Tutorial 1AshwinNo ratings yet
- EasyGreen ManualDocument33 pagesEasyGreen ManualpitoupitouNo ratings yet
- Fishblade RPGDocument1 pageFishblade RPGthe_doom_dudeNo ratings yet
- Wiring Diagram Obp 1 v2Document5 pagesWiring Diagram Obp 1 v2Jorge Luis Vera AlmeidaNo ratings yet
- Literature 1 Study GuideDocument7 pagesLiterature 1 Study GuideEs EsNo ratings yet
- MarketNexus Editor: Teri Buhl Character LetterDocument2 pagesMarketNexus Editor: Teri Buhl Character LetterTeri BuhlNo ratings yet
- Scan Sep 2, 2020Document1 pageScan Sep 2, 2020Taresh MittalNo ratings yet
- CV HannahDocument3 pagesCV HannahRoxan DosdosNo ratings yet
- OsteoporosisDocument57 pagesOsteoporosisViviViviNo ratings yet
- UITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioDocument9 pagesUITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioShamsyul AriffinNo ratings yet
- BS KashmiryatDocument67 pagesBS KashmiryatWaqas AhmedNo ratings yet
- Lesson 5 Classifications of CommunicationDocument48 pagesLesson 5 Classifications of CommunicationRovenick SinggaNo ratings yet
- Recording of Dying DeclarationDocument6 pagesRecording of Dying DeclarationsarayusindhuNo ratings yet
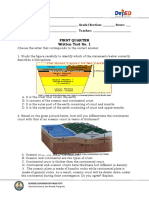
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- Dasakam 31-40Document16 pagesDasakam 31-40Puducode Rama Iyer RamachanderNo ratings yet
- A Case of Haemochromatosis and Diabetes A Missed OpportunityDocument111 pagesA Case of Haemochromatosis and Diabetes A Missed Opportunitymimran1974No ratings yet
- How to Launder Money in Real EstateDocument58 pagesHow to Launder Money in Real EstateSpeedyGonsalesNo ratings yet
- ACCT250-Auditing Course OutlineDocument7 pagesACCT250-Auditing Course OutlineammadNo ratings yet
- Tax 1Document351 pagesTax 1AbbyNo ratings yet
- Sustainable Farming FPO Promotes Natural AgricultureDocument4 pagesSustainable Farming FPO Promotes Natural AgricultureSHEKHAR SUMITNo ratings yet