You might also like
- Prognostic Role of Subclinical Left Ventricular Systolic Dysfunction Evaluated by Speckle-Tracking Echocardiography in Rheumatoid ArthritisDocument10 pagesPrognostic Role of Subclinical Left Ventricular Systolic Dysfunction Evaluated by Speckle-Tracking Echocardiography in Rheumatoid ArthritisEmanuel NavarreteNo ratings yet
- Christersson2022 Article ScreeningForBiomarkersAssociatDocument11 pagesChristersson2022 Article ScreeningForBiomarkersAssociatS FznsNo ratings yet
- Potter 2021Document12 pagesPotter 2021Paul CalbureanNo ratings yet
- Bolen2015 Article CardiacMRImagingInConstrictiveDocument8 pagesBolen2015 Article CardiacMRImagingInConstrictivesalikiqbalNo ratings yet
- Acs 33 241Document9 pagesAcs 33 241Ratna AyieNo ratings yet
- PVC Ablation in Non Ischaemic CMODocument8 pagesPVC Ablation in Non Ischaemic CMOZaraNo ratings yet
- 1 s2.0 S0735109700006902 MainDocument6 pages1 s2.0 S0735109700006902 MainEyal RobinsonNo ratings yet
- 07032501-Standard DDD PacingDocument3 pages07032501-Standard DDD PacingRobertoNo ratings yet
- Cardiac ValveDocument9 pagesCardiac Valveikbal rambalinoNo ratings yet
- New-Onset Supraventricular Arrhythmia During Septic Shock: Prevalence, Risk Factors and PrognosisDocument8 pagesNew-Onset Supraventricular Arrhythmia During Septic Shock: Prevalence, Risk Factors and PrognosisAhmad FahroziNo ratings yet
- Correlates and Long Term Implication of Left Ventricular Mechanical Dispersion by Tqo Dimensional Speckle Tracking EchocardiographyDocument9 pagesCorrelates and Long Term Implication of Left Ventricular Mechanical Dispersion by Tqo Dimensional Speckle Tracking EchocardiographyMarco Antonio Viera ArevaloNo ratings yet
- Application of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationDocument8 pagesApplication of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationSondang JasmineNo ratings yet
- Ebrahim 2021Document8 pagesEbrahim 2021wiyay34652ceoshubcomNo ratings yet
- Doshi 2005Document6 pagesDoshi 2005Luba D'AndreaNo ratings yet
- 4 PDFDocument15 pages4 PDFLivianty HukubunNo ratings yet
- Catheter Cardiovasc Interv 2021 May 27 Romeo FJDocument8 pagesCatheter Cardiovasc Interv 2021 May 27 Romeo FJFernando SousaNo ratings yet
- Circulation 1975 Burggraf 146 56Document12 pagesCirculation 1975 Burggraf 146 56Zikri Putra Lan LubisNo ratings yet
- Jurnal Mutiple StentDocument9 pagesJurnal Mutiple StentPrima Anggreini ArinNo ratings yet
- Article2017ICMBoissier DysfonctionVGSepticshockDocument10 pagesArticle2017ICMBoissier DysfonctionVGSepticshockenriquegarciagalianaNo ratings yet
- Equency of Right Ventricular InfarctionDocument4 pagesEquency of Right Ventricular InfarctionWeila dos Santos VieiraNo ratings yet
- 1 s2.0 S0002914922005355 MainDocument11 pages1 s2.0 S0002914922005355 MainRamona GhengheaNo ratings yet
- 998 FullDocument7 pages998 FullsilviaNo ratings yet
- Manuscript v5Document27 pagesManuscript v5Diego LowensteinNo ratings yet
- Essayagh Et Al 2021 The Mitral Annular Disjunction of Mitral Valve ProlapseDocument15 pagesEssayagh Et Al 2021 The Mitral Annular Disjunction of Mitral Valve Prolapsejesana.jes2No ratings yet
- Ehf2 13519Document10 pagesEhf2 13519Defriyan RamziNo ratings yet
- 1 s2.0 S0002914916305574 MainDocument6 pages1 s2.0 S0002914916305574 MainDavid Jimmy Kurniawan RejosaputroNo ratings yet
- 1 s2.0 S0002914915018445 MainDocument8 pages1 s2.0 S0002914915018445 MainFaomix de la HouseNo ratings yet
- J Jacc 2021 08 061Document11 pagesJ Jacc 2021 08 061Dhessy SusantoNo ratings yet
- Prognostic Significance of PVCS and Resting Heart RateDocument9 pagesPrognostic Significance of PVCS and Resting Heart RateLivianty HukubunNo ratings yet
- Bossi - Echocardiogric EvaluationDocument8 pagesBossi - Echocardiogric EvaluationSzendeNo ratings yet
- Troponina Guided Coronary ComputedDocument11 pagesTroponina Guided Coronary ComputedafFNo ratings yet
- AcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedDocument6 pagesAcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedWaldemar PiñaNo ratings yet
- Fux ECMODocument12 pagesFux ECMOPriya Nair MenonNo ratings yet
- Biomedicines 10 02407 v2Document13 pagesBiomedicines 10 02407 v2akinaNo ratings yet
- EE Pac Con FADocument6 pagesEE Pac Con FAGuillermo CenturionNo ratings yet
- Diltiazem in ANOCADocument12 pagesDiltiazem in ANOCAChristiaan VoslooNo ratings yet
- Prognostic Utility of Calcium Scoring As An Adjunct To Stress Myocardial Perfusion Scintigraphy in End-Stage Renal DiseaseDocument10 pagesPrognostic Utility of Calcium Scoring As An Adjunct To Stress Myocardial Perfusion Scintigraphy in End-Stage Renal DiseasePatricia CovarrubiasNo ratings yet
- F QRSDocument9 pagesF QRSaisyah hamzakirNo ratings yet
- Prognostic Implication of A Novel Right Ventricular Injury Score in Septic PatientsDocument9 pagesPrognostic Implication of A Novel Right Ventricular Injury Score in Septic PatientsKorejat KDNo ratings yet
- Lower Extremity Revascularization Using Directional AtherectomyDocument11 pagesLower Extremity Revascularization Using Directional AtherectomyEnrique San NorbertoNo ratings yet
- Ischemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesDocument6 pagesIschemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesIJAR JOURNALNo ratings yet
- JHLT Abstract 2020-1Document1 pageJHLT Abstract 2020-1G WNo ratings yet
- Setb 57 1 61 67 PDFDocument7 pagesSetb 57 1 61 67 PDFI Al WNo ratings yet
- Anticoagulation Resumption After Intracerebral HemorrhageDocument10 pagesAnticoagulation Resumption After Intracerebral HemorrhagesenkonenNo ratings yet
- Meta Analysis (Left Ventricular Unloading During Extracorporeal Membrane Oxygenation in Patients With Cardiogenic Shock) - JACC (2019)Document9 pagesMeta Analysis (Left Ventricular Unloading During Extracorporeal Membrane Oxygenation in Patients With Cardiogenic Shock) - JACC (2019)Sanchit ChawlaNo ratings yet
- Braverman Et Al. - 1991 - Cyclophosphamide Cardiotoxicity in Bone Marrow TraDocument9 pagesBraverman Et Al. - 1991 - Cyclophosphamide Cardiotoxicity in Bone Marrow Traaly alyNo ratings yet
- DTI Superposition PDFDocument7 pagesDTI Superposition PDFEtel SilvaNo ratings yet
- Jurnal PediatricDocument4 pagesJurnal PediatricJayantiNo ratings yet
- Right Ventricular Enlargement and Dysfunction Are Associated With Increased All-Cause Mortality in Hypertrophic CardiomyopathyDocument11 pagesRight Ventricular Enlargement and Dysfunction Are Associated With Increased All-Cause Mortality in Hypertrophic CardiomyopathySara Valentina GarciaNo ratings yet
- Jurnal InternalDocument10 pagesJurnal InternalseptikusumaNo ratings yet
- Hot Topics in Tetralogy of FallotDocument12 pagesHot Topics in Tetralogy of FallotqanitaNo ratings yet
- Leong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaDocument8 pagesLeong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaauliaNo ratings yet
- Cohorte Retrospectivda NOAF in CRITICSLLY ILLDocument8 pagesCohorte Retrospectivda NOAF in CRITICSLLY ILLARTURO YOSHIMAR LUQUE MAMANINo ratings yet
- A Randomized Controlled Trial CCMDocument10 pagesA Randomized Controlled Trial CCMAnonymous NeRC5JYiSNo ratings yet
- Shanghai Score System For Diagnosis of Brugada Syndrome PDFDocument7 pagesShanghai Score System For Diagnosis of Brugada Syndrome PDFFendy WellenNo ratings yet
- BLOCK HF Trial. JACC 2016Document10 pagesBLOCK HF Trial. JACC 2016Ernesto J. Rocha ReyesNo ratings yet
- CHF Dan CBFDocument5 pagesCHF Dan CBFRisky Ilona SaputraNo ratings yet
- Abdominal Aortic Calcification On A Plain X-Ray and The Relation With Significant Coronary Artery Disease in Asymptomatic Chronic Dialysis PatientsDocument7 pagesAbdominal Aortic Calcification On A Plain X-Ray and The Relation With Significant Coronary Artery Disease in Asymptomatic Chronic Dialysis PatientsArdiansyah Yolanda PutraNo ratings yet
- Impairment of Ventilatory Efficiency in Heart Failure: Prognostic ImpactDocument8 pagesImpairment of Ventilatory Efficiency in Heart Failure: Prognostic Impactabraham rumayaraNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Sex-Based Differences AutoinmunityDocument8 pagesSex-Based Differences AutoinmunityVallejo Romo Alberto CristianNo ratings yet
- High Prevalence of Altered Immunological Biomarkers in A TransgenderDocument5 pagesHigh Prevalence of Altered Immunological Biomarkers in A TransgenderVallejo Romo Alberto CristianNo ratings yet
- Investigating Sex Differences in T Regulatory Cells FromDocument15 pagesInvestigating Sex Differences in T Regulatory Cells FromVallejo Romo Alberto CristianNo ratings yet
- Gender Affirming Hormone Therapy Induces Specific DNA Methylation ChangesDocument34 pagesGender Affirming Hormone Therapy Induces Specific DNA Methylation ChangesVallejo Romo Alberto CristianNo ratings yet
- Gender Diverse and Inclusion in Investigation en InmunologyDocument13 pagesGender Diverse and Inclusion in Investigation en InmunologyVallejo Romo Alberto CristianNo ratings yet
- Atrial Infarction A Literature Review Laura Duque 2020Document8 pagesAtrial Infarction A Literature Review Laura Duque 2020Vallejo Romo Alberto CristianNo ratings yet
- Luis Fernando Pava MolanoDocument5 pagesLuis Fernando Pava MolanoVallejo Romo Alberto CristianNo ratings yet
- Vereckei TVDocument12 pagesVereckei TVVallejo Romo Alberto CristianNo ratings yet
- Chap22 PDFDocument9 pagesChap22 PDFSam CryshnaNo ratings yet
- Criterios de Barcelona 2020Document22 pagesCriterios de Barcelona 2020Vallejo Romo Alberto CristianNo ratings yet
- Wide Complex TachyDocument26 pagesWide Complex TachywongNo ratings yet
- TV Inducida Por FarmacosDocument3 pagesTV Inducida Por FarmacosVallejo Romo Alberto CristianNo ratings yet
- Algorithm accurately detects ventricular tachycardiaDocument10 pagesAlgorithm accurately detects ventricular tachycardiaVallejo Romo Alberto CristianNo ratings yet
- Taquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Document16 pagesTaquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Vallejo Romo Alberto CristianNo ratings yet
- Acute Coronary Syndromes PDF 66142023361477Document54 pagesAcute Coronary Syndromes PDF 66142023361477Vallejo Romo Alberto CristianNo ratings yet
- 202003324a EN JW Digital Program Flyer - p1 PDFDocument3 pages202003324a EN JW Digital Program Flyer - p1 PDFVallejo Romo Alberto CristianNo ratings yet
- Ultrasonido en El Paciente Crítico Daniel Lichtenstein PDFDocument33 pagesUltrasonido en El Paciente Crítico Daniel Lichtenstein PDFVallejo Romo Alberto CristianNo ratings yet
- Colchicina y COVID 19Document8 pagesColchicina y COVID 19Vallejo Romo Alberto CristianNo ratings yet
- Pondering The Atypicality of ARDS in COVID-19 Is A Distraction For The Bedside DoctorDocument2 pagesPondering The Atypicality of ARDS in COVID-19 Is A Distraction For The Bedside DoctorVallejo Romo Alberto CristianNo ratings yet
- Protocolo Taquicardia VentricularDocument9 pagesProtocolo Taquicardia VentricularOmar Díaz CuchoNo ratings yet
- 10 1097@CCM 0000000000003544Document7 pages10 1097@CCM 0000000000003544Vallejo Romo Alberto CristianNo ratings yet
- ESBG Financial Systems Difference EU-US PDFDocument12 pagesESBG Financial Systems Difference EU-US PDFDominiqueCarriouNo ratings yet
- Maruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationDocument4 pagesMaruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationHarshaNo ratings yet
- تركيب وتشغيل وحدات تكييف الهواءDocument49 pagesتركيب وتشغيل وحدات تكييف الهواءOmar NabilNo ratings yet
- Award 34509Document43 pagesAward 34509Brendon ChiaNo ratings yet
- RIZAL: INSPIRATION FOR A NEW GENERATIONDocument11 pagesRIZAL: INSPIRATION FOR A NEW GENERATIONErica B. DaclanNo ratings yet
- Power Over Ethernet - Wikipedia, The Free EncyclopediaDocument7 pagesPower Over Ethernet - Wikipedia, The Free EncyclopediaManitNo ratings yet
- Chapter 21 - Shock - Diagnosis and ManagementDocument10 pagesChapter 21 - Shock - Diagnosis and ManagementNeily Maulida UlfaNo ratings yet
- Dip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017Document2 pagesDip HIV Man (SA) Past Papers - 2015 2nd Semester 24-1-2017matenten100% (1)
- HZVDocument6 pagesHZVnurrozaqNo ratings yet
- Course 1 ProjectDocument6 pagesCourse 1 ProjectDhruvNo ratings yet
- Unit 5 - Lesson 1 - Understanding Hypothesis TestingDocument31 pagesUnit 5 - Lesson 1 - Understanding Hypothesis TestingJasper A. SANTIAGONo ratings yet
- Installing Juniper Router OS JunOS 10 1 in Qemu VM For GNS3Document4 pagesInstalling Juniper Router OS JunOS 10 1 in Qemu VM For GNS3Adrian Ionut NituNo ratings yet
- The Science and Art of DSGE ModellingDocument9 pagesThe Science and Art of DSGE ModellingkeyyongparkNo ratings yet
- Choose the Right Low Boy Trailer ModelDocument42 pagesChoose the Right Low Boy Trailer ModelOdlnayer AllebramNo ratings yet
- Strategic Planning Assignment - TescoDocument16 pagesStrategic Planning Assignment - TescoKayode Trinity Omosebi100% (1)
- Imeko WC 2012 TC21 O10Document5 pagesImeko WC 2012 TC21 O10mcastillogzNo ratings yet
- HW3 - Chapter 9-2Document3 pagesHW3 - Chapter 9-2Zachary MedeirosNo ratings yet
- Probability and Statistics. ASSIGNMENT 2Document5 pagesProbability and Statistics. ASSIGNMENT 2ByhiswillNo ratings yet
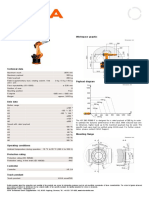
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Enquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerDocument7 pagesEnquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerNhi Hoàng Lê NguyễnNo ratings yet
- Emd MPC 543Document25 pagesEmd MPC 543jaskaran singhNo ratings yet
- Holzma PR Hob and Ex Linger Enu 18533Document7 pagesHolzma PR Hob and Ex Linger Enu 18533esfandiar232477No ratings yet
- Febelfin Academy - Exam RegulationsDocument9 pagesFebelfin Academy - Exam RegulationsGeoff ChapmanNo ratings yet
- Google Wakeword Detection 1 PDFDocument5 pagesGoogle Wakeword Detection 1 PDFÖzgür Bora GevrekNo ratings yet
- Resume Masroor 3Document3 pagesResume Masroor 3mohammad masroor zahid ullahNo ratings yet
- Interrogating Texts: Six Reading Habits To Develop in Your First Year at HarvardDocument2 pagesInterrogating Texts: Six Reading Habits To Develop in Your First Year at HarvardS I ZahidNo ratings yet
- Neurodegenerative Disorders of ChildhoodDocument51 pagesNeurodegenerative Disorders of ChildhoodPRONTO DIAGNOSTICNo ratings yet
- Mapeh-7pe Q2 Summative-TestDocument2 pagesMapeh-7pe Q2 Summative-TestVhannie AcquiatanNo ratings yet
- Flared Separable FittingDocument9 pagesFlared Separable FittingbenNo ratings yet
- Dual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band ScramblingDocument16 pagesDual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band Scramblingraja rishyantNo ratings yet