You might also like
- 4 575973715896959428Document13 pages4 575973715896959428Wahyu KarunaNo ratings yet
- Harrison SLEDocument11 pagesHarrison SLEpazucenaNo ratings yet
- Golden Dawn 2 9 The Moon BreathDocument4 pagesGolden Dawn 2 9 The Moon BreathF_RCNo ratings yet
- JCI78088Document6 pagesJCI78088Ardian AshadiNo ratings yet
- Sex-Based Differences AutoinmunityDocument8 pagesSex-Based Differences AutoinmunityVallejo Romo Alberto CristianNo ratings yet
- Semana 9 - Lupus PDFDocument12 pagesSemana 9 - Lupus PDFSheyla Osorio RamosNo ratings yet
- Semana 9 - Lupus PDFDocument12 pagesSemana 9 - Lupus PDFSheyla Osorio RamosNo ratings yet
- Experiment 12: Rheumatoid Factor Determination (Latex Slide Test)Document2 pagesExperiment 12: Rheumatoid Factor Determination (Latex Slide Test)Marjorie ColtingNo ratings yet
- Neuro-Inflammatory DisordersDocument7 pagesNeuro-Inflammatory DisordersInes StrenjaNo ratings yet
- 37 Aup EtalDocument8 pages37 Aup EtaleditorijmrhsNo ratings yet
- Netic Basis of AutoimmunityDocument9 pagesNetic Basis of AutoimmunityVasincu AlexandruNo ratings yet
- AR - Epidemiología y ParogeniaDocument11 pagesAR - Epidemiología y ParogeniamonseibanezbarraganNo ratings yet
- NIH Public Access: Estrogen Effects in Allergy and AsthmaDocument13 pagesNIH Public Access: Estrogen Effects in Allergy and AsthmaNoviantina 2017-24No ratings yet
- Human Autoimmune Diseases: A Comprehensive Update: ReviewDocument27 pagesHuman Autoimmune Diseases: A Comprehensive Update: Reviewkaren rinconNo ratings yet
- Sle and Infectous AgentsDocument7 pagesSle and Infectous AgentsAmany RadwanNo ratings yet
- Systemic Autoinflamatory DiseaseDocument10 pagesSystemic Autoinflamatory DiseaseJair Alexander Quintero PanucoNo ratings yet
- Endo GenusDocument5 pagesEndo Genuslabor baiturrahimNo ratings yet
- Journal of Population Therapeutics & Clinical PharmacologyDocument5 pagesJournal of Population Therapeutics & Clinical PharmacologyFrancis DhanarajNo ratings yet
- Pathogenesis and Clinical Aspects of Rheumatoid Arthritis: Ivan Padjen, Cem Gabay, Daniel AletahaDocument83 pagesPathogenesis and Clinical Aspects of Rheumatoid Arthritis: Ivan Padjen, Cem Gabay, Daniel AletahaPankaj VatsaNo ratings yet
- Xu J - Elevated Serum Levels of Transforming Growth Factor 1 in Epstein BarrDocument4 pagesXu J - Elevated Serum Levels of Transforming Growth Factor 1 in Epstein BarrmecyalvindaNo ratings yet
- Congenic Mice: Cutting Tools For Complex Immune Disorders: Ute C. Rogner and Philip AvnerDocument11 pagesCongenic Mice: Cutting Tools For Complex Immune Disorders: Ute C. Rogner and Philip AvnerJimit GandhiNo ratings yet
- Karagianni 2019Document10 pagesKaragianni 2019Fina AstinaNo ratings yet
- Menstrual Changes in Lupus Patients Using Immune-SuppressantsDocument8 pagesMenstrual Changes in Lupus Patients Using Immune-SuppressantsNisa UcilNo ratings yet
- EditorialDocument2 pagesEditorialsebastoto778No ratings yet
- 2020-Autoimmunity and Organ Damage in SLEDocument24 pages2020-Autoimmunity and Organ Damage in SLECinantya Meyta SariNo ratings yet
- Art 5Document4 pagesArt 5Emily YuliethNo ratings yet
- Frontiers in Neuroendocrinology: S.T. Ngo, F.J. Steyn, P.A. MccombeDocument23 pagesFrontiers in Neuroendocrinology: S.T. Ngo, F.J. Steyn, P.A. MccombeYudha RadistyoNo ratings yet
- Review: New Concepts in The Pathophysiology of Inflammatory Bowel DiseaseDocument11 pagesReview: New Concepts in The Pathophysiology of Inflammatory Bowel DiseaseReynalth Andrew Sinaga100% (1)
- Reviewing Immunoassay Interferences: Detecting and Resolving Erroneous ResultsDocument5 pagesReviewing Immunoassay Interferences: Detecting and Resolving Erroneous ResultsKartika ParamitaNo ratings yet
- JDM - Amezcua-Guerra Et Al 2017Document8 pagesJDM - Amezcua-Guerra Et Al 2017Ricardo Colín MartínezNo ratings yet
- Rheumatoid Arthritis: Andrew P. CopeDocument15 pagesRheumatoid Arthritis: Andrew P. CopesamNo ratings yet
- Review LESDocument16 pagesReview LESyoNo ratings yet
- envhper00522-0014Document5 pagesenvhper00522-0014Afaq AhmadNo ratings yet
- Atm 05 06 151Document3 pagesAtm 05 06 151Marius VoineaNo ratings yet
- Ad 26 526Document2 pagesAd 26 526tizziana carollaNo ratings yet
- Science Magazine, Issue 6644 (May 5, 2023)Document128 pagesScience Magazine, Issue 6644 (May 5, 2023)Kim LevrelNo ratings yet
- Discipline: B. Tech (Biotech) Module: BT 501 IV Semester: VDocument6 pagesDiscipline: B. Tech (Biotech) Module: BT 501 IV Semester: VsauravsarkarNo ratings yet
- Rheumatoid Arthritis and The Concept of Autoimmune DiseaseDocument5 pagesRheumatoid Arthritis and The Concept of Autoimmune DiseaseDORINNE KINDAONo ratings yet
- JGR 3 019Document7 pagesJGR 3 019patgarettNo ratings yet
- Serum Tumor Necrosis Factor Alpha and Gene Polymorphisms in Rheumatoid Arthritis Patients in Babylon Province, IraqDocument9 pagesSerum Tumor Necrosis Factor Alpha and Gene Polymorphisms in Rheumatoid Arthritis Patients in Babylon Province, IraqDr-Abdulsamie Hassan Alta'eeNo ratings yet
- Research ProposalDocument30 pagesResearch ProposalAmitabh RanjanNo ratings yet
- Warm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentDocument8 pagesWarm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentMishel PazmiñoNo ratings yet
- Eda JurnalDocument13 pagesEda JurnalekalapaleloNo ratings yet
- Patients Treated With The Pregnancy Immune Modulation in Multiple SclerosisDocument9 pagesPatients Treated With The Pregnancy Immune Modulation in Multiple SclerosisdeboratomeNo ratings yet
- PIIS1074761313004378Document14 pagesPIIS1074761313004378ZadorxsNo ratings yet
- Anti Thyroid AntibodyDocument16 pagesAnti Thyroid AntibodyFritz HaryadiNo ratings yet
- sirs carsDocument14 pagessirs carsJosé ChalcoNo ratings yet
- Thyroid-Associated Ophthalmopathy: ReviewDocument12 pagesThyroid-Associated Ophthalmopathy: Reviewkevin_jawanNo ratings yet
- Acel 13361Document15 pagesAcel 13361iva hullNo ratings yet
- En V58n5a22Document13 pagesEn V58n5a22M Nurshaffriaal RusdiNo ratings yet
- Anaphylaxis Diagnosis, TreatmentDocument6 pagesAnaphylaxis Diagnosis, TreatmentutifornaNo ratings yet
- Vanduin 2007Document7 pagesVanduin 2007arfikNo ratings yet
- Torres 2009Document4 pagesTorres 2009gaesca63No ratings yet
- P I B A: Ossible Mmunogenetic Asis For UtismDocument5 pagesP I B A: Ossible Mmunogenetic Asis For UtismHarshit AmbeshNo ratings yet
- Systemic Lupus ErythematosusDocument10 pagesSystemic Lupus ErythematosuszkxxyyNo ratings yet
- Etiology of Autoimmune Disease: Past, Present and Future: CommentaryDocument3 pagesEtiology of Autoimmune Disease: Past, Present and Future: Commentarydiaa skamNo ratings yet
- AIJ - TratamientoDocument5 pagesAIJ - TratamientomonseibanezbarraganNo ratings yet
- Immunological Basis of Infertility in AnimalsDocument13 pagesImmunological Basis of Infertility in AnimalsRamachandran Ram100% (3)
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementFrom EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouNo ratings yet
- Management of Infections in the Immunocompromised HostFrom EverandManagement of Infections in the Immunocompromised HostBrahm H. SegalNo ratings yet
- Immune Hematology: Diagnosis and Management of Autoimmune CytopeniasFrom EverandImmune Hematology: Diagnosis and Management of Autoimmune CytopeniasJenny M. DespotovicNo ratings yet
- Gender Affirming Hormone Therapy Induces Specific DNA Methylation ChangesDocument34 pagesGender Affirming Hormone Therapy Induces Specific DNA Methylation ChangesVallejo Romo Alberto CristianNo ratings yet
- Investigating Sex Differences in T Regulatory Cells FromDocument15 pagesInvestigating Sex Differences in T Regulatory Cells FromVallejo Romo Alberto CristianNo ratings yet
- Chap22 PDFDocument9 pagesChap22 PDFSam CryshnaNo ratings yet
- Gender Diverse and Inclusion in Investigation en InmunologyDocument13 pagesGender Diverse and Inclusion in Investigation en InmunologyVallejo Romo Alberto CristianNo ratings yet
- Criterios de Barcelona 2020Document22 pagesCriterios de Barcelona 2020Vallejo Romo Alberto CristianNo ratings yet
- Taquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Document16 pagesTaquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Vallejo Romo Alberto CristianNo ratings yet
- Vereckei TVDocument12 pagesVereckei TVVallejo Romo Alberto CristianNo ratings yet
- Atrial Infarction A Literature Review Laura Duque 2020Document8 pagesAtrial Infarction A Literature Review Laura Duque 2020Vallejo Romo Alberto CristianNo ratings yet
- Algorithm accurately detects ventricular tachycardiaDocument10 pagesAlgorithm accurately detects ventricular tachycardiaVallejo Romo Alberto CristianNo ratings yet
- TV Inducida Por FarmacosDocument3 pagesTV Inducida Por FarmacosVallejo Romo Alberto CristianNo ratings yet
- Luis Fernando Pava MolanoDocument5 pagesLuis Fernando Pava MolanoVallejo Romo Alberto CristianNo ratings yet
- 202003324a EN JW Digital Program Flyer - p1 PDFDocument3 pages202003324a EN JW Digital Program Flyer - p1 PDFVallejo Romo Alberto CristianNo ratings yet
- Voskoboinik2020 ABC SCOREDocument9 pagesVoskoboinik2020 ABC SCOREVallejo Romo Alberto CristianNo ratings yet
- Acute Coronary Syndromes PDF 66142023361477Document54 pagesAcute Coronary Syndromes PDF 66142023361477Vallejo Romo Alberto CristianNo ratings yet
- Wide Complex TachyDocument26 pagesWide Complex TachywongNo ratings yet
- Colchicina y COVID 19Document8 pagesColchicina y COVID 19Vallejo Romo Alberto CristianNo ratings yet
- 10 1097@CCM 0000000000003544Document7 pages10 1097@CCM 0000000000003544Vallejo Romo Alberto CristianNo ratings yet
- Protocolo Taquicardia VentricularDocument9 pagesProtocolo Taquicardia VentricularOmar Díaz CuchoNo ratings yet
- Pondering The Atypicality of ARDS in COVID-19 Is A Distraction For The Bedside DoctorDocument2 pagesPondering The Atypicality of ARDS in COVID-19 Is A Distraction For The Bedside DoctorVallejo Romo Alberto CristianNo ratings yet
- Ultrasonido en El Paciente Crítico Daniel Lichtenstein PDFDocument33 pagesUltrasonido en El Paciente Crítico Daniel Lichtenstein PDFVallejo Romo Alberto CristianNo ratings yet
- Fi & EiDocument3 pagesFi & EiPrasanna S Kulkarni100% (1)
- Shangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Document2 pagesShangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Salma FarooqNo ratings yet
- Matrox DSX Le4Document76 pagesMatrox DSX Le4doc docNo ratings yet
- Phychem Chapter 3 Part 1Document14 pagesPhychem Chapter 3 Part 1Skye DiazNo ratings yet
- SampleDocument8 pagesSampleAntônioNo ratings yet
- Impex Kitchen Appliances PDFDocument4 pagesImpex Kitchen Appliances PDFqwqw11No ratings yet
- Logicroof V-RP enDocument1 pageLogicroof V-RP enCristina DogariNo ratings yet
- Heliflex Hose CatalogueDocument119 pagesHeliflex Hose CatalogueAugustine DharmarajNo ratings yet
- Audit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaDocument10 pagesAudit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaSawaluddin SawalNo ratings yet
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- Kraby System 2018Document22 pagesKraby System 2018soga010178No ratings yet
- AstigmatismDocument1 pageAstigmatismAmmellya PutriNo ratings yet
- MIND - BODY RelationshipDocument18 pagesMIND - BODY RelationshipvishwabhashaNo ratings yet
- RTWP OptimisationHanFeedbackDocument31 pagesRTWP OptimisationHanFeedbackSeth Mawuli Dedzoe100% (1)
- Service Manual: Freestanding Cooling Double Door ARC 2140Document5 pagesService Manual: Freestanding Cooling Double Door ARC 2140Sergio ZapataNo ratings yet
- Calculation of Carbon Footprint: HouseDocument3 pagesCalculation of Carbon Footprint: HouseUmut ÇağırganNo ratings yet
- 07 - Structural Organisation in AnimalsDocument31 pages07 - Structural Organisation in AnimalsKamala Kannan XANo ratings yet
- Steel Grid StructureDocument2 pagesSteel Grid StructureKusum RawatNo ratings yet
- Physical Activity Guidelines Advisory Committee ReportDocument683 pagesPhysical Activity Guidelines Advisory Committee Reportyitz22100% (1)
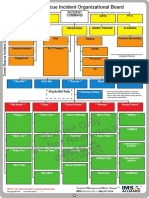
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- LEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019Document18 pagesLEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019kaito kurabaNo ratings yet
- Understanding and Quantifying Mountain TourismDocument84 pagesUnderstanding and Quantifying Mountain TourismfloridNo ratings yet
- BMK PDFDocument8 pagesBMK PDFHuỳnh Minh SángNo ratings yet
- Drawing and Reading Structural FormulasDocument12 pagesDrawing and Reading Structural FormulasVy Nguyen100% (1)
- IRIScan Book Executive 3 PDFDocument86 pagesIRIScan Book Executive 3 PDFssamplingNo ratings yet
- Air Sentry - Energy Statement App 3 Dessicant and Filters PDFDocument20 pagesAir Sentry - Energy Statement App 3 Dessicant and Filters PDFEsteban Fernando Meza IbacetaNo ratings yet
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
- Dog Cake Recipe For Dozer's Birthday! - RecipeTin EatsDocument36 pagesDog Cake Recipe For Dozer's Birthday! - RecipeTin EatsZyreen Kate CataquisNo ratings yet
- Blackmer Pump Parts ListDocument2 pagesBlackmer Pump Parts ListFelipe Ignacio PaillavilNo ratings yet