You might also like
- CASESHEETPHARMDDocument6 pagesCASESHEETPHARMDSai SharathNo ratings yet
- Mechanics of Mandibular MovementDocument5 pagesMechanics of Mandibular MovementOpris PetruNo ratings yet
- The Pharmaceutics and Compounding LaboratoryDocument20 pagesThe Pharmaceutics and Compounding Laboratoryهبة سالم100% (1)
- CP 3Document18 pagesCP 3Rubina MasihNo ratings yet
- Case Study Guide What Is A Case Study in Nursing?Document5 pagesCase Study Guide What Is A Case Study in Nursing?Angel CauilanNo ratings yet
- CP 4Document18 pagesCP 4Rubina MasihNo ratings yet
- Nejmcpc 2115850Document9 pagesNejmcpc 2115850masonicpgsNo ratings yet
- Case 3-2022 - A 14-Year-Old Boy With Fever, Joint Pain, and Abdominal CrampingDocument9 pagesCase 3-2022 - A 14-Year-Old Boy With Fever, Joint Pain, and Abdominal CrampingPierre Pradel100% (1)
- Case FormatDocument7 pagesCase FormatSheila SimanganNo ratings yet
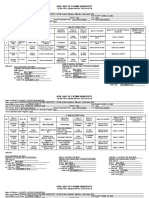
- Ofelia L. Mendoza Maternity and General Hospital Nurses NotesDocument3 pagesOfelia L. Mendoza Maternity and General Hospital Nurses NotesMia Zabelle V. PascualNo ratings yet
- New FormatDocument5 pagesNew FormatedzNo ratings yet
- Intravenous and Blood Transfusion SetDocument6 pagesIntravenous and Blood Transfusion SetMia Zabelle V. PascualNo ratings yet
- Digital Learner'S Worksheet: Student Nameraphael Chino Aragon Date: InstitutionDocument67 pagesDigital Learner'S Worksheet: Student Nameraphael Chino Aragon Date: InstitutionRAPHAEL CHINO ARAGONNo ratings yet
- Mariano Marcos State University: College of Health SciencesDocument3 pagesMariano Marcos State University: College of Health SciencesJoshua GonzalesNo ratings yet
- Form 1Document6 pagesForm 1Jusmine Rose MundaNo ratings yet
- University of Rizal SystemDocument10 pagesUniversity of Rizal SystemJann Marvin Rabaja AbingNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Obstetric Case AnalysisDocument2 pagesObstetric Case AnalysisDud AccNo ratings yet
- Tsuruta 2005Document2 pagesTsuruta 2005chrislxt1No ratings yet
- NDH-NS3 NCPDocument3 pagesNDH-NS3 NCPJonathan R. YadaoNo ratings yet
- BSN2B G4 Case-2Document16 pagesBSN2B G4 Case-2Reyzel PahunaoNo ratings yet
- NSVD CaseDocument8 pagesNSVD CaseMARK JASON DIAZNo ratings yet
- Case Scenario No. 3 Intrapartum Labor Stage 1Document2 pagesCase Scenario No. 3 Intrapartum Labor Stage 1Ice BEARNo ratings yet
- Patient'S Record: University of Northern PhilippinesDocument21 pagesPatient'S Record: University of Northern PhilippinesCezanne CruzNo ratings yet
- FDAR ChartingDocument50 pagesFDAR ChartingNathaniel PulidoNo ratings yet
- Group 2 OBDocument27 pagesGroup 2 OBReymart EstebanNo ratings yet
- FECALYSISDocument1 pageFECALYSISSyan ApuyanNo ratings yet
- Jose R. Reyes Memorial Medical Center Department of Pediatrics Clinical History FormDocument2 pagesJose R. Reyes Memorial Medical Center Department of Pediatrics Clinical History FormAnonymous Zqe563ZNo ratings yet
- Intervention 2Document8 pagesIntervention 2Jomie Rose ReyesNo ratings yet
- Kawasaki Disease: Nur Intan Sartika Supervisor: Dr. Hotber E R Pasaribu, Sp. A (K) M.SiDocument21 pagesKawasaki Disease: Nur Intan Sartika Supervisor: Dr. Hotber E R Pasaribu, Sp. A (K) M.SiIntan AdeNo ratings yet
- Vital InformationDocument4 pagesVital InformationCristina L. JaysonNo ratings yet
- Asthma Case StudyDocument39 pagesAsthma Case StudyYzel Vasquez AdavanNo ratings yet
- Fdar LP 6Document4 pagesFdar LP 6Krizzia Mae ColladoNo ratings yet
- Pulmonary EdemaDocument23 pagesPulmonary EdemaELISION OFFICIALNo ratings yet
- TH ND ST RDDocument5 pagesTH ND ST RDJOANA KRIS CABALTERANo ratings yet
- Page 3 6 MHR PRESCREEN QUESTIONNAIREDocument5 pagesPage 3 6 MHR PRESCREEN QUESTIONNAIREMark Joel AguilaNo ratings yet
- ABELLA, AMSON - M2 Lesson 2A Learning Outcomes AssessmentDocument2 pagesABELLA, AMSON - M2 Lesson 2A Learning Outcomes AssessmentJULIANE MARIE ABELLANo ratings yet
- Our Lady of Fatima UniversityDocument6 pagesOur Lady of Fatima UniversityJane Veronica PatricioNo ratings yet
- Group F - Nursing Kardex Written OutputDocument7 pagesGroup F - Nursing Kardex Written OutputMatty JolbitadoNo ratings yet
- PRC FORM To Be SubmittedDocument6 pagesPRC FORM To Be SubmittedCarlos NiñoNo ratings yet
- CHN Bag Sample LetterDocument1 pageCHN Bag Sample LetterMei MeiNo ratings yet
- Case No. Name of Mother AGE Address Hospital Date of Delivery Supervising Physician Handled/ AssistedDocument1 pageCase No. Name of Mother AGE Address Hospital Date of Delivery Supervising Physician Handled/ AssistedArman Carl DulayNo ratings yet
- Phototheraphy ADocument41 pagesPhototheraphy AhaneyumiiiNo ratings yet
- Care of Mother, Child, & Adolescent Lec: PartographDocument6 pagesCare of Mother, Child, & Adolescent Lec: PartographBardiaga JmayNo ratings yet
- Adobe Scan 08 Jan 2024Document1 pageAdobe Scan 08 Jan 2024Marie Faith DumpaNo ratings yet
- Journal 4-5Document2 pagesJournal 4-5api-546041650No ratings yet
- Care Plan On CataractDocument36 pagesCare Plan On CataractPATEL NEHAKUMARI VIMALBHAINo ratings yet
- Genotype Phenotype Analysis in A Family Carrying Truncating Mutations in The Titin GeneDocument5 pagesGenotype Phenotype Analysis in A Family Carrying Truncating Mutations in The Titin GeneL ANo ratings yet
- R-Mẫu KSK đi du học MỹDocument6 pagesR-Mẫu KSK đi du học MỹTrần Gia NghĩaNo ratings yet
- Nov 30 Dec 2 Case Study Module 1Document7 pagesNov 30 Dec 2 Case Study Module 1Kristian Karl Bautista Kiw-isNo ratings yet
- Surgical Safety Checklist: Feu-Dr. Nicanor Reyes Medical Foundation Medical ReyesDocument1 pageSurgical Safety Checklist: Feu-Dr. Nicanor Reyes Medical Foundation Medical Reyesnictan 14No ratings yet
- Blank Clinical Log - Spring 2nd HalfDocument2 pagesBlank Clinical Log - Spring 2nd HalfEileenNo ratings yet
- Pre-Natal Care: Jennifer F. Aficial Man. RNDocument21 pagesPre-Natal Care: Jennifer F. Aficial Man. RNshana ferrerNo ratings yet
- Loryang CaseconDocument8 pagesLoryang CaseconRichard AbucayNo ratings yet
- Actual Delivery FormDocument1 pageActual Delivery FormGilyan ZaniahNo ratings yet
- Burn CsDocument23 pagesBurn CsMASII100% (1)
- 0322 - AgoniaDocument8 pages0322 - AgoniaBel CortezNo ratings yet
- 29 17case StudyDocument47 pages29 17case StudyLa YannaNo ratings yet
- Nejm CASODocument9 pagesNejm CASOJuan Esteban Rincon HuertasNo ratings yet
- CASE STUDY ABRUPTIO PLACENTA BSN 2 H For Printing NA FINAL NAaaaaaaDocument36 pagesCASE STUDY ABRUPTIO PLACENTA BSN 2 H For Printing NA FINAL NAaaaaaaisaacdarylNo ratings yet
- Spina Bifida CaseanalysisDocument26 pagesSpina Bifida Caseanalysisaasimon2466cabNo ratings yet
- Childhood Obesity. Rista. Insufficiently Adequate Response.From EverandChildhood Obesity. Rista. Insufficiently Adequate Response.No ratings yet
- CHN Module 1Document34 pagesCHN Module 1Don Maur ValeteNo ratings yet
- Theories Settings of CHNDocument73 pagesTheories Settings of CHNDon Maur ValeteNo ratings yet
- Unit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingDocument140 pagesUnit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingDon Maur ValeteNo ratings yet
- Nutrition Diagnosis and Plan of CareDocument4 pagesNutrition Diagnosis and Plan of CareDon Maur ValeteNo ratings yet
- Definition of Nursing InformaticsDocument29 pagesDefinition of Nursing InformaticsDon Maur Valete100% (1)
- THERAPEUTIC DIET StudentsDocument18 pagesTHERAPEUTIC DIET StudentsDon Maur ValeteNo ratings yet
- Breast Feeding: Formula PreparationDocument15 pagesBreast Feeding: Formula PreparationDon Maur ValeteNo ratings yet
- Nutri Last LectDocument22 pagesNutri Last LectDon Maur ValeteNo ratings yet
- NUTRITION AND DIET THERAPHY ModuleDocument11 pagesNUTRITION AND DIET THERAPHY ModuleDon Maur ValeteNo ratings yet
- Different Fields of NursingDocument6 pagesDifferent Fields of NursingDon Maur ValeteNo ratings yet
- NUTRITION ACROSS THE LIFESPAN StudentsDocument32 pagesNUTRITION ACROSS THE LIFESPAN StudentsDon Maur ValeteNo ratings yet
- Community Health Nursing WEEK-1-AND-2Document23 pagesCommunity Health Nursing WEEK-1-AND-2Don Maur ValeteNo ratings yet
- School Timing CircularDocument2 pagesSchool Timing Circularabhi_chakravarti20005881No ratings yet
- Gene TherapiesDocument15 pagesGene Therapiesenfanat23No ratings yet
- Pediatric Department Faculty of MedicineDocument100 pagesPediatric Department Faculty of MedicineIrfanNo ratings yet
- Wipro Limited Karan 13Document15 pagesWipro Limited Karan 13Kinjal BhanushaliNo ratings yet
- Anterior Cruciate Ligament InjuryDocument30 pagesAnterior Cruciate Ligament InjuryyohanNo ratings yet
- Concurrent Validity and Clinical Utility of The HCR-20V3Document9 pagesConcurrent Validity and Clinical Utility of The HCR-20V3JC BarrientosNo ratings yet
- Ask Questions About C.P.RDocument5 pagesAsk Questions About C.P.RAnonymous FCOOcnNo ratings yet
- Datasheet - EXPLORE': Policy DetailsDocument4 pagesDatasheet - EXPLORE': Policy DetailsAbdul Wahab ZafarNo ratings yet
- Personality Disorders - A Brief OverviewDocument2 pagesPersonality Disorders - A Brief OverviewMaria- AndreeaNo ratings yet
- Sex Education in Schools Argumentative EssayDocument4 pagesSex Education in Schools Argumentative Essayfira100% (1)
- Drug Proving Project InvestigationsDocument8 pagesDrug Proving Project InvestigationsJayNo ratings yet
- Six Ways To Refresh Your MindDocument3 pagesSix Ways To Refresh Your MindBhupesh D. SahareNo ratings yet
- Henry Dunant Solferino Icrc-002-0361 PDFDocument150 pagesHenry Dunant Solferino Icrc-002-0361 PDFgorazd100% (1)
- GRCHRT Girls 24LW 9210Document1 pageGRCHRT Girls 24LW 9210Stephen GregorNo ratings yet
- Glossary of Environmental TermsDocument6 pagesGlossary of Environmental TermsSalman HaroonNo ratings yet
- A Progress of Herbal Finish (Aloe Vera & Neem) in Infant Tank Tops in Mother's View PointDocument6 pagesA Progress of Herbal Finish (Aloe Vera & Neem) in Infant Tank Tops in Mother's View PointEditor IJTSRDNo ratings yet
- Functions of Public HealthDocument30 pagesFunctions of Public Healthteklay100% (1)
- Volume 12 Number 2Document179 pagesVolume 12 Number 2evi.setianingsihNo ratings yet
- Waste Management Laws PDFDocument7 pagesWaste Management Laws PDFrohit kumar0% (1)
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- 23-1. Overview of Articulation Materials and Methods For The Prosthodontic Patient PDFDocument13 pages23-1. Overview of Articulation Materials and Methods For The Prosthodontic Patient PDFPablo Gutiérrez Da VeneziaNo ratings yet
- Change of Dentin Surface by Low-Power Irradiation - OcredDocument5 pagesChange of Dentin Surface by Low-Power Irradiation - OcredBogdan HohaNo ratings yet
- Shoulder Arthroscopy: How To Succeed!Document119 pagesShoulder Arthroscopy: How To Succeed!Btoaew BtoaewNo ratings yet
- Virology The Study of VirusesDocument45 pagesVirology The Study of Virusesdawoodabdullah56100% (2)
- Level: Subject Group: Subject:: Senior High School Core Subject Physical Education and Health (Grade 12)Document1 pageLevel: Subject Group: Subject:: Senior High School Core Subject Physical Education and Health (Grade 12)CIELITO ANNE INOBAYANo ratings yet
- Making Brands Matter in Turbulent Times:: How To Steer Brands Through A CrisisDocument31 pagesMaking Brands Matter in Turbulent Times:: How To Steer Brands Through A Crisischiranjeeb mitraNo ratings yet
- NATUSDocument3 pagesNATUSΠΑΝΤΕΛΗΣ ΧΟΥΡΙΔΗΣNo ratings yet
- An Introduction To Genetic Engineering: Third Edition Desmond S. T. Nicholl 2008Document12 pagesAn Introduction To Genetic Engineering: Third Edition Desmond S. T. Nicholl 2008Rosi Nurbaeti PutriNo ratings yet