You might also like
- Reinforced Concrete Design Solution Manual 7th Edition PDFDocument5 pagesReinforced Concrete Design Solution Manual 7th Edition PDFEdmond Orena BautistaNo ratings yet
- Galeo Wa430-6 PDFDocument1,612 pagesGaleo Wa430-6 PDFWalter100% (1)
- PnemoniaDocument4 pagesPnemoniadhavalNo ratings yet
- Uworld EndocrineDocument211 pagesUworld Endocrineهنادي رازمNo ratings yet
- Liver Function Tests Diagnostic GuideDocument2 pagesLiver Function Tests Diagnostic GuideostarburstoNo ratings yet
- Pathogens of The Vagina-Annie Espinosa - This Is The Revised VersionDocument1 pagePathogens of The Vagina-Annie Espinosa - This Is The Revised VersionMicroposterNo ratings yet
- Respiratory Tract InfectionsDocument1 pageRespiratory Tract InfectionsShannon RamsumairNo ratings yet
- Megaloblastic Anemias: Dept of Medicine AcmsDocument71 pagesMegaloblastic Anemias: Dept of Medicine Acmskunal ghosh100% (1)
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Creatin. Creatin. Creatin. Creatin. Creatin. CreatinDocument2 pagesCreatin. Creatin. Creatin. Creatin. Creatin. CreatinEna PaparićNo ratings yet
- Renal Cell Carcinoma Risk Factors & TypesDocument1 pageRenal Cell Carcinoma Risk Factors & TypesBobet ReñaNo ratings yet
- Lower Genital Infections GuideDocument2 pagesLower Genital Infections Guidecbac1990No ratings yet
- Protozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreDocument32 pagesProtozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreFort SalvadorNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- Hematology Lectures 1 5 DR - TuyDocument10 pagesHematology Lectures 1 5 DR - TuyMiguel Cuevas DolotNo ratings yet
- Pathogens of The Female Reproductive System - Leah NechamkinDocument1 pagePathogens of The Female Reproductive System - Leah NechamkinMicroposterNo ratings yet
- Kaposis Sarcoma: Denis NahabweDocument32 pagesKaposis Sarcoma: Denis NahabwexilcomNo ratings yet
- Graves' Disease Signs and ManagementDocument11 pagesGraves' Disease Signs and ManagementManisha Sekaran Muniandy100% (1)
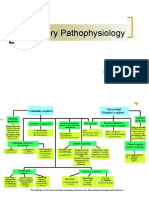
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- 20 Pathoma Skin DisordersDocument10 pages20 Pathoma Skin Disordersn alawiNo ratings yet
- PleuraDocument6 pagesPleuraameerabest100% (1)
- Kidney NewDocument4 pagesKidney NewParth BhayanaNo ratings yet
- Cryptococcosis: The Fungal Infection of Lungs and BrainDocument17 pagesCryptococcosis: The Fungal Infection of Lungs and BrainKarthick AnbuNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Treatment and Classification of Heart FailureDocument2 pagesTreatment and Classification of Heart FailureShannon RamsumairNo ratings yet
- Pathology B - Gastrointestinal Tract (Esguerra, 2015) PDFDocument18 pagesPathology B - Gastrointestinal Tract (Esguerra, 2015) PDFJem QuintoNo ratings yet
- Patho. Reviewer On Cellular InjuryDocument21 pagesPatho. Reviewer On Cellular InjurySeff CausapinNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Medicine 6.1b Approach To Cancer Patients - FernandoDocument7 pagesMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausNo ratings yet
- Chart - WBC DisordersDocument1 pageChart - WBC DisordersSamuel RothschildNo ratings yet
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- LeukemiasDocument8 pagesLeukemiasharideepNo ratings yet
- For More Details Please Visit Our WebsiteDocument25 pagesFor More Details Please Visit Our Websiteajie354No ratings yet
- Structural Biology of HIVDocument31 pagesStructural Biology of HIVLaura TapiaNo ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Heart BNHADocument13 pagesHeart BNHAX OloGyNo ratings yet
- Kidney Physiology (Q & A)Document28 pagesKidney Physiology (Q & A)ramadan100% (1)
- Boards - Gen AnaDocument26 pagesBoards - Gen AnaJoyce EbolNo ratings yet
- The Basal Ganglia Mashehabat@just - Edu.joDocument62 pagesThe Basal Ganglia Mashehabat@just - Edu.joSaddamix AL OmariNo ratings yet
- Dr. A. Samy TAG Bone Diseases - 1Document2 pagesDr. A. Samy TAG Bone Diseases - 1Herato MenaNo ratings yet
- Valvular Heart DseDocument8 pagesValvular Heart DseJane Pineda CuraNo ratings yet
- Heamtology Reviewer (Midterm)Document15 pagesHeamtology Reviewer (Midterm)Johney DoeNo ratings yet
- Red Blood Cell Disorders Anemia: Anemia Is A Laboratory DiagnosisDocument3 pagesRed Blood Cell Disorders Anemia: Anemia Is A Laboratory DiagnosisAnonymous 8hJAATBNo ratings yet
- Handouts Integumentary Sys Sp11 B201Document7 pagesHandouts Integumentary Sys Sp11 B201Kelly TrainorNo ratings yet
- Acute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmDocument1 pageAcute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmAudreySlitNo ratings yet
- 4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangDocument4 pages4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangMiel Raphael AranillaNo ratings yet
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramNo ratings yet
- Protein Synth Inhibs Target Bact RibosomeDocument61 pagesProtein Synth Inhibs Target Bact RibosomegirNo ratings yet
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisNo ratings yet
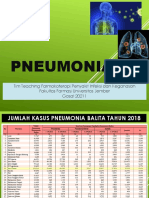
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Document67 pagesPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariNo ratings yet
- Protein Metab 2 Dra. SantosDocument7 pagesProtein Metab 2 Dra. SantosMelissa SalayogNo ratings yet
- Pathology B - Gastrointestinal Tract (Esguerra, 2015)Document18 pagesPathology B - Gastrointestinal Tract (Esguerra, 2015)Ars MoriendiNo ratings yet
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- Understanding Toxic Epidermal NecrolysisDocument13 pagesUnderstanding Toxic Epidermal NecrolysisHend AbdallaNo ratings yet
- Acute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzDocument30 pagesAcute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzNilay ChatterjeeNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- RabiesDocument10 pagesRabiesWinda LiraNo ratings yet
- Kidney TumorsDocument15 pagesKidney TumorsJose SirittNo ratings yet
- Kidney & Urothelial TumoursDocument74 pagesKidney & Urothelial Tumoursjames20123No ratings yet
- Bladder tumor pathology guideDocument11 pagesBladder tumor pathology guidePankaj DubeyNo ratings yet
- Prostate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillanceDocument2 pagesProstate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillancePankaj DubeyNo ratings yet
- Book IRCTC ticket onlineDocument2 pagesBook IRCTC ticket onlineHimanshu GuptaNo ratings yet
- Book IRCTC ticket onlineDocument2 pagesBook IRCTC ticket onlineHimanshu GuptaNo ratings yet
- Probability As A General Concept Can Be Defined As The Chance of An Event OccurDocument14 pagesProbability As A General Concept Can Be Defined As The Chance of An Event OccurMuhammad Adnan KhalidNo ratings yet
- Trắc nghiệm phần thì trong tiếng anh tổng hợp with keysDocument3 pagesTrắc nghiệm phần thì trong tiếng anh tổng hợp with keysMs ArmyNo ratings yet
- Prospectus PDFDocument40 pagesProspectus PDFSony ManojNo ratings yet
- Agilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentsDocument6 pagesAgilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentshendraprimaNo ratings yet
- VOLLEYBALL HISTORY AND RULESDocument12 pagesVOLLEYBALL HISTORY AND RULESJennybelle MolinaNo ratings yet
- Epidemiology and Etiology of Peptic Ulcer DiseaseDocument5 pagesEpidemiology and Etiology of Peptic Ulcer DiseaseDeepali Mahajan ChaudhariNo ratings yet
- Fishing and Hunting Gear From Osseous Raw Materials in The Early Neolithic From SerbiaDocument12 pagesFishing and Hunting Gear From Osseous Raw Materials in The Early Neolithic From SerbiaDanaGrujićNo ratings yet
- Environmental AuditingDocument27 pagesEnvironmental Auditinghitman agent 47No ratings yet
- Types of DisasterDocument22 pagesTypes of DisasterKirstin del CarmenNo ratings yet
- Gigabyte Z590 Gaming-XDocument52 pagesGigabyte Z590 Gaming-XjanchixnsNo ratings yet
- Id Card SoftwareDocument6 pagesId Card SoftwareAlli RaniNo ratings yet
- FM 4 Fluid Kinematics CompleteDocument48 pagesFM 4 Fluid Kinematics Completeالياس يونس مرغلانيNo ratings yet
- BS SMP 7-8-9 Bab B. Inggris Sec. Text (Reading) (SB - Descriptive Text)Document5 pagesBS SMP 7-8-9 Bab B. Inggris Sec. Text (Reading) (SB - Descriptive Text)TeresaAvilla Ayuning BudiCayestuNo ratings yet
- Parts List - KTZ411-63Document4 pagesParts List - KTZ411-63Mahmoud ElboraeNo ratings yet
- B. Inggris Kels IXDocument4 pagesB. Inggris Kels IXANHAS ADVERTISINGNo ratings yet
- Herman Pardamean Hutabarat: Mechanical EngineerDocument3 pagesHerman Pardamean Hutabarat: Mechanical EngineerHerman HutabaratNo ratings yet
- Mci 2005Document3 pagesMci 2005Christos LeptokaridisNo ratings yet
- MAYTAG MDE28PNCGW0 TechSheet-W10589718-RevADocument8 pagesMAYTAG MDE28PNCGW0 TechSheet-W10589718-RevAAngel MartinezNo ratings yet
- Bsczo 201Document280 pagesBsczo 201ishfaqqqNo ratings yet
- Races of HyruleDocument99 pagesRaces of HyruleScrindlemorpNo ratings yet
- Four Course Meal Plan and BudgetDocument5 pagesFour Course Meal Plan and BudgetPemphoNo ratings yet
- Case 1Document6 pagesCase 1Rewaa MerwadNo ratings yet
- Postdoctoral Research Associate in Functional Organic MaterialsDocument6 pagesPostdoctoral Research Associate in Functional Organic MaterialsTheo GazisNo ratings yet
- CS601 - Machine Learning - Unit 2 - Notes - 1672759753Document14 pagesCS601 - Machine Learning - Unit 2 - Notes - 1672759753mohit jaiswalNo ratings yet
- Monorail HC Overhead Track Scale: Technical ManualDocument30 pagesMonorail HC Overhead Track Scale: Technical ManualRicardo Vazquez SalinasNo ratings yet
- Tips On Fatigue - NAVWEPS 00-25-559Document123 pagesTips On Fatigue - NAVWEPS 00-25-559Mark Evan SalutinNo ratings yet
- ConMed v. Cosmescu Et. Al.Document28 pagesConMed v. Cosmescu Et. Al.PriorSmartNo ratings yet
- Python Programming For Mechanical EngineersDocument93 pagesPython Programming For Mechanical EngineerslucianoprocopioNo ratings yet