You might also like
- Steven Taylor - The Psychology of Pandemics - Preparing For The Next Global Outbreak of Infectious Disease-Cambridge Scholars Publishing (2019) PDFDocument179 pagesSteven Taylor - The Psychology of Pandemics - Preparing For The Next Global Outbreak of Infectious Disease-Cambridge Scholars Publishing (2019) PDFCaroline Barroso100% (4)
- Epidemiologic Basis For TB Control. Rieder. 1999Document164 pagesEpidemiologic Basis For TB Control. Rieder. 1999Percy Hugo Flores MerinoNo ratings yet
- 9th R.LDocument101 pages9th R.LWilliam Tac anNo ratings yet
- (Libribook - Com) Introduction To Clinical Infectious Diseases A Problem-Based Approach 1st EditionDocument465 pages(Libribook - Com) Introduction To Clinical Infectious Diseases A Problem-Based Approach 1st EditionDaoud IssaNo ratings yet
- Mental Health Support for Coronavirus Staff, Volunteers & CommunitiesDocument14 pagesMental Health Support for Coronavirus Staff, Volunteers & CommunitiesGlenn Kenneth Esguerra IINo ratings yet
- Swine Flu WhitepaperDocument95 pagesSwine Flu WhitepaperPatrick Savalle100% (1)
- Psychiatry of Pandemics: A Mental Health Response to Infection OutbreakFrom EverandPsychiatry of Pandemics: A Mental Health Response to Infection OutbreakDamir HuremovićNo ratings yet
- HPV-Infection and Cancers of the Skin - Diagnostics and TherapyFrom EverandHPV-Infection and Cancers of the Skin - Diagnostics and TherapyRating: 5 out of 5 stars5/5 (1)
- Pediatric OI 2Document176 pagesPediatric OI 2muinateebNo ratings yet
- Vaccine DesigneDocument702 pagesVaccine DesigneItrux jonathan cisnerosNo ratings yet
- The Wisdom of COVID-19: How to Rejuvenate, Reclaim Hope, and Heal in the New Post-Pandemic WorldFrom EverandThe Wisdom of COVID-19: How to Rejuvenate, Reclaim Hope, and Heal in the New Post-Pandemic WorldNo ratings yet
- Immunity: The Science of Staying Well—The Definitive Guide to Caring for Your Immune SystemFrom EverandImmunity: The Science of Staying Well—The Definitive Guide to Caring for Your Immune SystemRating: 3.5 out of 5 stars3.5/5 (2)
- The Wuhan Coronavirus: Survival Manual and Concise Guide to COVID-19 (Symptoms, Outbreak, and Prevention in 2020)From EverandThe Wuhan Coronavirus: Survival Manual and Concise Guide to COVID-19 (Symptoms, Outbreak, and Prevention in 2020)No ratings yet
- Issue 3 Dementia Psychology: A Cognitive Psychology, Biological Psychology and Neuropsychology Guide To Dementia: Psychology Worlds, #3From EverandIssue 3 Dementia Psychology: A Cognitive Psychology, Biological Psychology and Neuropsychology Guide To Dementia: Psychology Worlds, #3No ratings yet
- Preparedness For A High-Impact Respiratory Pathogen Pandemic PDFDocument84 pagesPreparedness For A High-Impact Respiratory Pathogen Pandemic PDFchinzsteelNo ratings yet
- COVID-19: A Devil's Choice: How We Got Here. How We'll Get OutFrom EverandCOVID-19: A Devil's Choice: How We Got Here. How We'll Get OutRating: 3 out of 5 stars3/5 (2)
- Beyond Mental Illness: Transform the Labels Transform a LifeFrom EverandBeyond Mental Illness: Transform the Labels Transform a LifeNo ratings yet
- Morales J. The Innate Immune System in Health... Vol 1. 2022Document328 pagesMorales J. The Innate Immune System in Health... Vol 1. 2022Philip Rodríguez GarcíaNo ratings yet
- The Bird Flu Mastery Bible: Your Blueprint For Complete Bird Flu Demystified ManagementFrom EverandThe Bird Flu Mastery Bible: Your Blueprint For Complete Bird Flu Demystified ManagementNo ratings yet
- AI in Clinical Practice: A Guide to Artificial Intelligence and Digital MedicineFrom EverandAI in Clinical Practice: A Guide to Artificial Intelligence and Digital MedicineNo ratings yet
- Boosting Immunity: Creating Wellness NaturallyFrom EverandBoosting Immunity: Creating Wellness NaturallyLen Saputo, MDRating: 4.5 out of 5 stars4.5/5 (4)
- Preview - Microbiology Nuts BoltsDocument67 pagesPreview - Microbiology Nuts Boltsshakil ahmed100% (3)
- The Swine Flu Mastery Bible: Your Blueprint for Complete Swine Flu ManagementFrom EverandThe Swine Flu Mastery Bible: Your Blueprint for Complete Swine Flu ManagementNo ratings yet
- Infection Prevention in Schools and ChildcareDocument105 pagesInfection Prevention in Schools and ChildcareRose AzuikeNo ratings yet
- Summary of Plague of Corruption: by Judy Mikovits and Kent Heckenlively - Restoring Faith in the Promise of Science - A Comprehensive SummaryFrom EverandSummary of Plague of Corruption: by Judy Mikovits and Kent Heckenlively - Restoring Faith in the Promise of Science - A Comprehensive SummaryNo ratings yet
- Curing our Ills: The psychology of chronic disease risk, experience and care in AfricaFrom EverandCuring our Ills: The psychology of chronic disease risk, experience and care in AfricaNo ratings yet
- The Practice of Predictive Analytics in Healthcare - by Gopalakrishna PalemDocument27 pagesThe Practice of Predictive Analytics in Healthcare - by Gopalakrishna PalemGopalakrishna Palem100% (1)
- Science and the Media: Delgado's Brave Bulls and the Ethics of Scientific DisclosureFrom EverandScience and the Media: Delgado's Brave Bulls and the Ethics of Scientific DisclosureNo ratings yet
- Journal of Affective Disorders: Giulio Perugi, Elie Hantouche, Giulia Vannucchi, Olavo PintoDocument15 pagesJournal of Affective Disorders: Giulio Perugi, Elie Hantouche, Giulia Vannucchi, Olavo PintoLuigi Maria PandolfiNo ratings yet
- The Coronavirus Conspiracy: An Exercise in Mass Fear and Mind ControlFrom EverandThe Coronavirus Conspiracy: An Exercise in Mass Fear and Mind ControlNo ratings yet
- Animal and Translational Models for CNS Drug Discovery: Psychiatric DisordersFrom EverandAnimal and Translational Models for CNS Drug Discovery: Psychiatric DisordersRobert A. McArthurNo ratings yet
- Getting Risk Right: Understanding the Science of Elusive Health RisksFrom EverandGetting Risk Right: Understanding the Science of Elusive Health RisksNo ratings yet
- Living with Dementia: Neuroethical Issues and International PerspectivesFrom EverandLiving with Dementia: Neuroethical Issues and International PerspectivesVeljko DubljevićNo ratings yet
- The Shingles Mastery Bible: Your Blueprint For Complete Shingles ManagementFrom EverandThe Shingles Mastery Bible: Your Blueprint For Complete Shingles ManagementNo ratings yet
- Rethinking Herd Immunity and Compulsory VaccinationDocument48 pagesRethinking Herd Immunity and Compulsory VaccinationGiada MoscatelloNo ratings yet
- Communicating Science and Managing the Coronavirus PandemicFrom EverandCommunicating Science and Managing the Coronavirus PandemicNo ratings yet
- The Flu Mastery Bible: Your Blueprint for Complete Flu ManagementFrom EverandThe Flu Mastery Bible: Your Blueprint for Complete Flu ManagementNo ratings yet
- SZL2111 PDFDocument153 pagesSZL2111 PDFoscarNo ratings yet
- Clinical Manual Preventioin MentalDocument440 pagesClinical Manual Preventioin MentalimilagiNo ratings yet
- Surprising Truths Behind the Coronavirus PandemicFrom EverandSurprising Truths Behind the Coronavirus PandemicRating: 5 out of 5 stars5/5 (1)
- Dead Wrong: Diagnosing and Treating Healthcare's Misinformation IllnessFrom EverandDead Wrong: Diagnosing and Treating Healthcare's Misinformation IllnessNo ratings yet
- PrisonofficersVERSION NUEVADocument32 pagesPrisonofficersVERSION NUEVAFARID TORRESNo ratings yet
- The Origin of Chronic Inflammatory Systemic Diseases and their SequelaeFrom EverandThe Origin of Chronic Inflammatory Systemic Diseases and their SequelaeNo ratings yet
- François Villon PoemsDocument20 pagesFrançois Villon PoemsBassem KamelNo ratings yet
- Kate Chopin's Story of an Hour: An Analysis of Irony and Women's RolesDocument22 pagesKate Chopin's Story of an Hour: An Analysis of Irony and Women's RolesBassem Kamel100% (1)
- Modernity and Its CriticsDocument13 pagesModernity and Its CriticsBassem Kamel100% (1)
- Dominant and Subaltern Voices in A Modest Proposal - A Postcolonial ReadingDocument5 pagesDominant and Subaltern Voices in A Modest Proposal - A Postcolonial ReadingBassem KamelNo ratings yet
- John Stuart Mill - Subjection-Of-Women - Notable-ExcerptsDocument2 pagesJohn Stuart Mill - Subjection-Of-Women - Notable-ExcerptsBassem KamelNo ratings yet
- BALLADS DONE INTO ENGLISH FROM THE French - Francois VillonDocument51 pagesBALLADS DONE INTO ENGLISH FROM THE French - Francois VillonBassem KamelNo ratings yet
- From Girl To Goddess The Heroines JourneDocument8 pagesFrom Girl To Goddess The Heroines JourneBassem KamelNo ratings yet
- "A Modest Proposal": By: Jonathan SwiftDocument12 pages"A Modest Proposal": By: Jonathan SwiftBassem KamelNo ratings yet
- Queer Theory: January 2008Document4 pagesQueer Theory: January 2008Ashish RanjanNo ratings yet
- Mythic Thought TextbookDocument73 pagesMythic Thought TextbookBassem KamelNo ratings yet
- Empress The Astonishing Reign of Nur JaDocument5 pagesEmpress The Astonishing Reign of Nur JaLakshmipriya P SanthoshNo ratings yet
- Posthumanist Literature?: July 2015Document17 pagesPosthumanist Literature?: July 2015Bassem KamelNo ratings yet
- Beyond Words For All Its WorthDocument44 pagesBeyond Words For All Its WorthBassem KamelNo ratings yet
- A Guide To Research Proposal and Thesis Writing PDFDocument52 pagesA Guide To Research Proposal and Thesis Writing PDFYasser HaddouNo ratings yet
- George LaturaDocument6 pagesGeorge LaturaBassem KamelNo ratings yet
- 3 Positive CBT ExercisesDocument23 pages3 Positive CBT ExercisesBassem Kamel100% (1)
- Before Athens - Early Popular Government in Phoenician and Greek City StatesDocument12 pagesBefore Athens - Early Popular Government in Phoenician and Greek City StatesBassem KamelNo ratings yet
- Whispers of LoveDocument6 pagesWhispers of LoveBassem KamelNo ratings yet
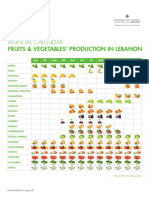
- Annual Calendar Fruits and VegetablesDocument1 pageAnnual Calendar Fruits and VegetablesBassem KamelNo ratings yet
- Elimination Diet EGuideDocument14 pagesElimination Diet EGuideViolet VioletNo ratings yet
- Behaviour Change Start Kit July 2019Document10 pagesBehaviour Change Start Kit July 2019Bassem KamelNo ratings yet
- What Is A NationDocument11 pagesWhat Is A Nationapi-270964392No ratings yet
- Who Is OpheliaDocument104 pagesWho Is OpheliaNamanNo ratings yet
- The Akashic Reading Guide - W4Document9 pagesThe Akashic Reading Guide - W4Priyanka SareenNo ratings yet
- 365-Daily-Health 101 Natural Remedies SecretsDocument47 pages365-Daily-Health 101 Natural Remedies SecretsBassem Kamel100% (1)
- Excerpt From Apollo S Arrow The Profound and Enduring Impact of Coronavirus On The Way We Live by Nicholas ChristakisDocument4 pagesExcerpt From Apollo S Arrow The Profound and Enduring Impact of Coronavirus On The Way We Live by Nicholas ChristakisBassem KamelNo ratings yet
- Brain Supplement Guide PDFDocument3 pagesBrain Supplement Guide PDFMashu MazzNo ratings yet
- Kahlil Gibran: Christopher BuckDocument18 pagesKahlil Gibran: Christopher BuckBassem KamelNo ratings yet
- Peeters - Dying and Rising GodsDocument3 pagesPeeters - Dying and Rising GodsBassem KamelNo ratings yet
- Elimination Diet EGuideDocument14 pagesElimination Diet EGuideViolet VioletNo ratings yet
- Effective Treatment of Rosacea Using Intense Pulsed LightDocument5 pagesEffective Treatment of Rosacea Using Intense Pulsed LightVo Ha Phuong NguyenNo ratings yet
- Midgut Volvulus 2018Document2 pagesMidgut Volvulus 2018zzzNo ratings yet
- Infectious Bronchitis in Broiler - Veterinaria DigitalDocument3 pagesInfectious Bronchitis in Broiler - Veterinaria DigitalMahesh KajagarNo ratings yet
- Australia Modified Karnofsky Performance ScaleDocument1 pageAustralia Modified Karnofsky Performance ScaleSirish ExpertNo ratings yet
- Cif AfpDocument2 pagesCif Afpninzah wanzahNo ratings yet
- Chickenpo X: Presented By:-Priya Yadav Roll No 02 2 Yeat BSC Nursing (H) College of Nursing Dr. RML HospitalDocument41 pagesChickenpo X: Presented By:-Priya Yadav Roll No 02 2 Yeat BSC Nursing (H) College of Nursing Dr. RML HospitalNikita JangraNo ratings yet
- John Paterson - The Bowel NosodesDocument16 pagesJohn Paterson - The Bowel NosodesDr Gayatri B IyerNo ratings yet
- 2023 Free 120Document65 pages2023 Free 120Edmund BlackadderNo ratings yet
- CHN Priorities Health DeficitsDocument6 pagesCHN Priorities Health DeficitsMika SaldañaNo ratings yet
- Submitted By: Amrita Mandal Subject: Yoga Assignment IiDocument5 pagesSubmitted By: Amrita Mandal Subject: Yoga Assignment IiAmrita MandalNo ratings yet
- Associação Da Ingestão de Glúten Nos Primeiros 5 Anos de Vida e A Incidencia de Doença CeliacaDocument10 pagesAssociação Da Ingestão de Glúten Nos Primeiros 5 Anos de Vida e A Incidencia de Doença CeliacaAna Beatriz SpagollaNo ratings yet
- TATALAKSANA PROGNOSIS Cushing SyndromeDocument13 pagesTATALAKSANA PROGNOSIS Cushing SyndromeFirda RidhayantiNo ratings yet
- Baveno 7Document16 pagesBaveno 7Mihai-Marian RuseiNo ratings yet
- ISLAB P2 - Anti-Streptolysin ODocument4 pagesISLAB P2 - Anti-Streptolysin ODanielle Anne LambanNo ratings yet
- 1-Aarogyam B + Covid Ab IgG - PO3827226873-180Document16 pages1-Aarogyam B + Covid Ab IgG - PO3827226873-180Rohit PandeyNo ratings yet
- Endodontic MicrobiologyDocument49 pagesEndodontic MicrobiologyEshal MuzaffarNo ratings yet
- Systematic Review of Differential Reinforcement of Alternative Behavior Without Extinction For Individuals With AutismDocument24 pagesSystematic Review of Differential Reinforcement of Alternative Behavior Without Extinction For Individuals With AutismVictor Martin CobosNo ratings yet
- Betnovate Scalp Solution Reduces Scalp ConditionsDocument7 pagesBetnovate Scalp Solution Reduces Scalp ConditionsdindaikaputriNo ratings yet
- CDC Facilities Covid-19 Screening: TODAY'S DATEDocument2 pagesCDC Facilities Covid-19 Screening: TODAY'S DATEpandijaiNo ratings yet
- Gautam PHD Dissertation 2013Document129 pagesGautam PHD Dissertation 2013sorinaNo ratings yet
- Las 5Document26 pagesLas 5kateNo ratings yet
- National Health Policy and PlanDocument92 pagesNational Health Policy and PlanChetan BhattaNo ratings yet
- Best Varicose Vein Treatment in ChennaiDocument5 pagesBest Varicose Vein Treatment in ChennaiLaser Vein ClinicNo ratings yet
- Quiz Critical CareDocument15 pagesQuiz Critical CareSuma AhmadNo ratings yet
- Pengaruh Varietas Dan Umur Tanaman Berbeda Terhadap Jumlah Populasi Dan Tingkat Serangan Hama Dan Penyakit Pisang (Musa SP.) Di Kabupaten SukabumiDocument8 pagesPengaruh Varietas Dan Umur Tanaman Berbeda Terhadap Jumlah Populasi Dan Tingkat Serangan Hama Dan Penyakit Pisang (Musa SP.) Di Kabupaten SukabumiAdil NugrohoNo ratings yet
- Childhood and Adolescent DisordersDocument60 pagesChildhood and Adolescent DisordersGolda MeboyaNo ratings yet
- Activity 7 - GARCES 109LECDocument10 pagesActivity 7 - GARCES 109LECSherlyn Miranda GarcesNo ratings yet
- Data Collection in EpidemiologyDocument32 pagesData Collection in EpidemiologyOlivier MakengoNo ratings yet
- Oral Patho Test 1Document11 pagesOral Patho Test 1Vijay K PatelNo ratings yet
- Final Blue Chip - OldDocument42 pagesFinal Blue Chip - OldAnusha SrivastavaNo ratings yet