You might also like
- MCQs ANS 2Document7 pagesMCQs ANS 2M Imran Sajid0% (1)
- Parasympathetic Nervous System DrugsDocument38 pagesParasympathetic Nervous System DrugsJon Corpuz AggasidNo ratings yet
- MCQ Base For Final Exam PreparationDocument131 pagesMCQ Base For Final Exam PreparationPurwa Rane100% (1)
- Definitions and classifications of muscle relaxantsDocument42 pagesDefinitions and classifications of muscle relaxantsMirza Shaharyar BaigNo ratings yet
- Pharmacology Exam 1 - Multiple ChoiceDocument13 pagesPharmacology Exam 1 - Multiple ChoiceNida Ridzuan50% (2)
- NMJ Blocking Agents GuideDocument69 pagesNMJ Blocking Agents Guidevvb_frndNo ratings yet
- Anticholinesterase: PHARMACOLOGY PPT by Dr. Geraldine CorporalDocument4 pagesAnticholinesterase: PHARMACOLOGY PPT by Dr. Geraldine Corporaltaco cat100% (1)
- Clinical Toxicology: MANOR Review CenterDocument24 pagesClinical Toxicology: MANOR Review CenterChia Jose100% (1)
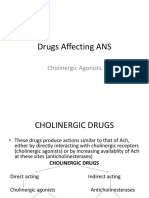
- Cholinergic AgonistsDocument25 pagesCholinergic AgonistsRahul VadlapatlaNo ratings yet
- Drugs Affecting ANS: Cholinergic AgonistsDocument25 pagesDrugs Affecting ANS: Cholinergic AgonistsAjay SinghNo ratings yet
- Cholinergic Agonist: (Direct Acting)Document31 pagesCholinergic Agonist: (Direct Acting)Shaukat HayatNo ratings yet
- Cholinergic System: Play A Significant Role in Termination of Acetylcholine's Effect in The SynapseDocument7 pagesCholinergic System: Play A Significant Role in Termination of Acetylcholine's Effect in The SynapseWilliam BufNo ratings yet
- PHARMACOLOGY LECTURES CHOLINERGIC MECHANISMS DR THERESA JOHN Sent To BSC SEP 20 2021Document33 pagesPHARMACOLOGY LECTURES CHOLINERGIC MECHANISMS DR THERESA JOHN Sent To BSC SEP 20 2021Ebenezer SamuelNo ratings yet
- 3.Ghafez-Cholinergic Neurotransmission and Related Drugs-2022Document40 pages3.Ghafez-Cholinergic Neurotransmission and Related Drugs-2022yasmin.rahmany03No ratings yet
- The Cholinergic System - PART 1Document6 pagesThe Cholinergic System - PART 1docsNo ratings yet
- Cholinergic Agonists: Prepared by: Sevan M. Rustum 07512491694 يسيردتلا رجفلا دهعمDocument41 pagesCholinergic Agonists: Prepared by: Sevan M. Rustum 07512491694 يسيردتلا رجفلا دهعمAhmed MohamadNo ratings yet
- Anticholinergic AgentsDocument36 pagesAnticholinergic AgentsNicole GalvezNo ratings yet
- Sosiologi KesehatanDocument62 pagesSosiologi KesehatanLucy WijayaNo ratings yet
- Choline RG Ics AbbreviatedDocument84 pagesCholine RG Ics AbbreviatedYousef JafarNo ratings yet
- Cholinergic Agonists and AntagonistsDocument750 pagesCholinergic Agonists and AntagonistsClarissa MaglalangNo ratings yet
- Cholinergic Drugs Parasympathomimetic Drugs Mechanism of ActionDocument8 pagesCholinergic Drugs Parasympathomimetic Drugs Mechanism of ActionanaNo ratings yet
- Cholinergic Agonist: By: Aditya AryaDocument57 pagesCholinergic Agonist: By: Aditya AryaJhung Manda SupaNo ratings yet
- #06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2Document66 pages#06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2tasnemaldaherNo ratings yet
- Cholinergic AgonistsDocument18 pagesCholinergic Agonistsbassist1089No ratings yet
- Al Ayen Universirty Faculty of Dentistry: Atropine DropDocument10 pagesAl Ayen Universirty Faculty of Dentistry: Atropine Dropاصاله رياض سرحان ساجتNo ratings yet
- Parasympathomimetics: Directly and Indirectly Acting DrugsDocument26 pagesParasympathomimetics: Directly and Indirectly Acting DrugsFlorenz GatchalianNo ratings yet
- Cholinomimetic DrugsDocument44 pagesCholinomimetic DrugsMohamed Abdi Baffo100% (1)
- Cholinergic drugs-BPTDocument39 pagesCholinergic drugs-BPTHUZAIFA YAMAANNo ratings yet
- Anticholinergic Drugs: Atropine, Scopolamine, GlycopyrrolateDocument7 pagesAnticholinergic Drugs: Atropine, Scopolamine, GlycopyrrolateLourdes RamírezNo ratings yet
- Neuropharma AntidementiaDocument29 pagesNeuropharma AntidementiaKeanne Paula AmamanglonNo ratings yet
- 1B Cholinergics and Anticholinergics Drug - StudentDocument41 pages1B Cholinergics and Anticholinergics Drug - StudentAlyanna Hope TondoNo ratings yet
- Materi KolinergikDocument62 pagesMateri KolinergikWira KrisnaNo ratings yet
- Cholinergic TransmissionDocument43 pagesCholinergic TransmissionAjay SinghNo ratings yet
- Updated-Autonomic Nervous SystemDocument84 pagesUpdated-Autonomic Nervous Systems.zainabtanweerNo ratings yet
- Cholinergic Antagonists GuideDocument49 pagesCholinergic Antagonists GuideGde Ananda ArmanditaNo ratings yet
- Cholinoceptors Activating Drugs.Document48 pagesCholinoceptors Activating Drugs.Kate EvangelistaNo ratings yet
- 5 Cholinergic AgonistDocument53 pages5 Cholinergic AgonistLoai Mohammed IssaNo ratings yet
- NEUROMUSCULAR BLOCKING AGENTSDocument26 pagesNEUROMUSCULAR BLOCKING AGENTSblessing akataNo ratings yet
- Pharma 2 Collective SummaryDocument44 pagesPharma 2 Collective Summaryمسعودة سعدNo ratings yet
- Unit 3 Drugs Acting of Autonomic Nervous System: StructureDocument12 pagesUnit 3 Drugs Acting of Autonomic Nervous System: StructureSwapnilPagareNo ratings yet
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- PHS 221Document18 pagesPHS 221tewogbadeomobuwajo005No ratings yet
- The Cholinergic Antagonists: PharmacologyDocument5 pagesThe Cholinergic Antagonists: PharmacologyDr-Dalya ShakirNo ratings yet
- Cholinergic AntagonistsDocument18 pagesCholinergic AntagonistsApurba Sarker Apu100% (1)
- Las PharmacologyDocument19 pagesLas Pharmacologyfrancialronnel69No ratings yet
- Cholinergic Antagonists: DR - Ch. Shanmukha Sai RaghavDocument12 pagesCholinergic Antagonists: DR - Ch. Shanmukha Sai RaghavShanmukh SaiNo ratings yet
- Pharmacology of Cholinomimetics BDSDocument34 pagesPharmacology of Cholinomimetics BDSDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Autonomics and CNS PlusDocument131 pagesAutonomics and CNS PlusMiguel TolentinoNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFferhanmu419No ratings yet
- Cholinergic DrugsDocument29 pagesCholinergic DrugsYashasv BhatnagarNo ratings yet
- Anticholinergic Drugs: Mechanisms and Clinical UsesDocument39 pagesAnticholinergic Drugs: Mechanisms and Clinical UsesDr.Biswajit jenaNo ratings yet
- Al-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonDocument42 pagesAl-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonAsdar LeaqerNo ratings yet
- Pharma Nca1 Notes MidtermDocument8 pagesPharma Nca1 Notes MidtermAICEL A. ABILNo ratings yet
- Neuromuscular Blocking Drugs: Mechanisms and Clinical UsesDocument5 pagesNeuromuscular Blocking Drugs: Mechanisms and Clinical UsesTherese Jane TiradorNo ratings yet
- Anticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCADocument5 pagesAnticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCAMarinaNo ratings yet
- Acetylcholinesterase InhibitorDocument11 pagesAcetylcholinesterase InhibitorAssassin's j :uNo ratings yet
- Unit 3 MC PDFDocument24 pagesUnit 3 MC PDFvanithaNo ratings yet
- ANS Pharmacology DCM 2.1Document115 pagesANS Pharmacology DCM 2.1cyber secNo ratings yet
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- Drugs Acting On Autonomic GangliaDocument9 pagesDrugs Acting On Autonomic GangliaDita Hasni100% (1)
- Organophosphate Poisoning GuidelineDocument5 pagesOrganophosphate Poisoning Guidelinelamoleverde9297No ratings yet
- Case Studies PharmacologyDocument6 pagesCase Studies PharmacologyZaigham HammadNo ratings yet
- ANTICHOLINERGIC GROUP 7 PharmDocument21 pagesANTICHOLINERGIC GROUP 7 PharmDavid MharkNo ratings yet
- Antibiotik Resiten3Document1 pageAntibiotik Resiten3Via EkawatiNo ratings yet
- Understanding the Autonomic Nervous SystemDocument56 pagesUnderstanding the Autonomic Nervous SystemMarsh MelloNo ratings yet
- Research Methods GuideDocument11 pagesResearch Methods GuideMarsh MelloNo ratings yet
- Unesco - Eolss Sample Chapters: Radiochemical TechniquesDocument10 pagesUnesco - Eolss Sample Chapters: Radiochemical TechniquesMarsh MelloNo ratings yet
- Unesco - Eolss Sample Chapters: Radiochemical TechniquesDocument10 pagesUnesco - Eolss Sample Chapters: Radiochemical TechniquesMarsh MelloNo ratings yet
- Toc PDFDocument11 pagesToc PDFArangaNo ratings yet
- 7 - CholinergicsDocument10 pages7 - CholinergicsRaunaq Singh RatraNo ratings yet
- Lecture 4. CholinomimeticsDocument23 pagesLecture 4. CholinomimeticssharenNo ratings yet
- General Pharmacology MCQ: 1. The Science Which Deals With The Drug and Their Action On Human Body Is CalledDocument274 pagesGeneral Pharmacology MCQ: 1. The Science Which Deals With The Drug and Their Action On Human Body Is CalledAmritesh singh thakurNo ratings yet
- List of Common Drugs and Their AntidotesDocument2 pagesList of Common Drugs and Their AntidotesMourian AmanNo ratings yet
- Characteristics and uses of cholinomimetic drugs and cholinesterase inhibitorsDocument5 pagesCharacteristics and uses of cholinomimetic drugs and cholinesterase inhibitorsAassh DcmbrNo ratings yet
- Anticholinesterase AgentsDocument11 pagesAnticholinesterase AgentsEric AryantoNo ratings yet
- Antidotes and Their UsesDocument3 pagesAntidotes and Their UsesAbdul SalamNo ratings yet
- Prescription Writing for Cleft Lip Repair ComplicationsDocument8 pagesPrescription Writing for Cleft Lip Repair ComplicationsJasper PanosoNo ratings yet
- Clinical Toxicology Page 1 of 10: TH TH TH THDocument10 pagesClinical Toxicology Page 1 of 10: TH TH TH THKitkat Casacop100% (1)
- Study QuestionsDocument5 pagesStudy QuestionsasemNo ratings yet
- Cholinergic DrugsDocument22 pagesCholinergic Drugsmug ashNo ratings yet
- Materi KolinergikDocument62 pagesMateri KolinergikWira KrisnaNo ratings yet
- Cholinergic drugs-BPTDocument39 pagesCholinergic drugs-BPTHUZAIFA YAMAANNo ratings yet
- Anticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCADocument5 pagesAnticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCAMarinaNo ratings yet
- Alkaloids For UndergraduateDocument80 pagesAlkaloids For Undergraduatempiirwe ramadhanNo ratings yet
- Cholinergic AgentDocument22 pagesCholinergic AgentRx Ram JadhavNo ratings yet
- Drugs Affecting the Autonomic Nervous SystemDocument6 pagesDrugs Affecting the Autonomic Nervous SystemNoriko MatsumotoNo ratings yet
- Cholinergic System Model Questions & AnswersDocument45 pagesCholinergic System Model Questions & AnswersDr.U.P.Rathnakar.MD.DIH.PGDHM100% (5)
- MCQS ANS 03 Sol PDFDocument4 pagesMCQS ANS 03 Sol PDFSamir Rekha Mukund Joshi100% (1)
- Parasympathomimetic AgentsDocument26 pagesParasympathomimetic Agentsrushikesh ugaleNo ratings yet
- Percy Lavon JulianDocument6 pagesPercy Lavon JulianVictorica MaloneyNo ratings yet
- Do PharmaDocument143 pagesDo PharmacpNo ratings yet
- Pharmacology of Autonomic Nervous System 2013Document166 pagesPharmacology of Autonomic Nervous System 2013Adimera TsehayeNo ratings yet
- Frog Rectus AbdominisDocument76 pagesFrog Rectus AbdominisAdhiraj KakkarNo ratings yet