You might also like
- A Beginner's Guide To Layer Farming - LivestockingDocument38 pagesA Beginner's Guide To Layer Farming - LivestockingAmine Laribi100% (1)
- Skeletal Muscle RelaxantsDocument34 pagesSkeletal Muscle RelaxantsLohithNo ratings yet
- HK VTC 25-11-2006 Medicinal MushroomsDocument31 pagesHK VTC 25-11-2006 Medicinal MushroomsdeepthikuppuswamyNo ratings yet
- Drugs Used in CcuDocument169 pagesDrugs Used in CcuAnusha Verghese100% (3)
- Human PapillomavirusDocument5 pagesHuman PapillomavirusSofiaLopezNo ratings yet
- Definitions and classifications of muscle relaxantsDocument42 pagesDefinitions and classifications of muscle relaxantsMirza Shaharyar BaigNo ratings yet
- Prepare Your Own Chicken FeedDocument4 pagesPrepare Your Own Chicken FeedVijay Jaybhaye100% (1)
- Inclusions HematologyDocument3 pagesInclusions HematologyMurreh100% (3)
- Below Knee and Through Knee Prosthesis GuideDocument4 pagesBelow Knee and Through Knee Prosthesis GuideClang TejadaNo ratings yet
- 2 (1) - 1Document66 pages2 (1) - 1ahmed hotyNo ratings yet
- Case Study On BurnsDocument16 pagesCase Study On BurnsRoanne Lagua100% (2)
- Cholinergic Agonists: Prepared by: Sevan M. Rustum 07512491694 يسيردتلا رجفلا دهعمDocument41 pagesCholinergic Agonists: Prepared by: Sevan M. Rustum 07512491694 يسيردتلا رجفلا دهعمAhmed MohamadNo ratings yet
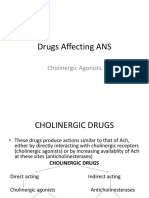
- Drugs Affecting ANS: Cholinergic AgonistsDocument25 pagesDrugs Affecting ANS: Cholinergic AgonistsAjay SinghNo ratings yet
- 5 Cholinergic AgonistDocument53 pages5 Cholinergic AgonistLoai Mohammed IssaNo ratings yet
- 3.Ghafez-Cholinergic Neurotransmission and Related Drugs-2022Document40 pages3.Ghafez-Cholinergic Neurotransmission and Related Drugs-2022yasmin.rahmany03No ratings yet
- Cholinomimetic DrugsDocument33 pagesCholinomimetic DrugsMarsh MelloNo ratings yet
- Sosiologi KesehatanDocument62 pagesSosiologi KesehatanLucy WijayaNo ratings yet
- Cholinergic AgonistsDocument25 pagesCholinergic AgonistsRahul VadlapatlaNo ratings yet
- Cholinergic AgonistsDocument18 pagesCholinergic Agonistsbassist1089No ratings yet
- Updated-Autonomic Nervous SystemDocument84 pagesUpdated-Autonomic Nervous Systems.zainabtanweerNo ratings yet
- The Cholinergic System - PART 1Document6 pagesThe Cholinergic System - PART 1docsNo ratings yet
- Cholinergic Agonist: By: Aditya AryaDocument57 pagesCholinergic Agonist: By: Aditya AryaJhung Manda SupaNo ratings yet
- #06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2Document66 pages#06-Cholinoceptor-Activating-Cholinesterase-Inh-Drugs - v2tasnemaldaherNo ratings yet
- Cholinergic Drugs Parasympathomimetic Drugs Mechanism of ActionDocument8 pagesCholinergic Drugs Parasympathomimetic Drugs Mechanism of ActionanaNo ratings yet
- PHS 221Document18 pagesPHS 221tewogbadeomobuwajo005No ratings yet
- ANS Pharmacology DCM 2.1Document115 pagesANS Pharmacology DCM 2.1cyber secNo ratings yet
- Direct Acting Cholinomimetics - BSN - 23Document28 pagesDirect Acting Cholinomimetics - BSN - 23KAMAU FRANCIS GATHUTHINo ratings yet
- Cholinergic DrugsDocument29 pagesCholinergic DrugsYashasv BhatnagarNo ratings yet
- Cholinergic drugs-BPTDocument39 pagesCholinergic drugs-BPTHUZAIFA YAMAANNo ratings yet
- Parasympathomimetics: Directly and Indirectly Acting DrugsDocument26 pagesParasympathomimetics: Directly and Indirectly Acting DrugsFlorenz GatchalianNo ratings yet
- Skeletal Muscle Relaxants 1Document21 pagesSkeletal Muscle Relaxants 1pooja sureshNo ratings yet
- Neuromuscular BlockersDocument49 pagesNeuromuscular Blockerssongo sorshimaNo ratings yet
- Chapter 5 (Cholinergic Antagonists)Document42 pagesChapter 5 (Cholinergic Antagonists)Aneeza AhmadNo ratings yet
- 2 - ParasympathomimeticsDocument99 pages2 - ParasympathomimeticsHamid Hussain HamidNo ratings yet
- Pharma Nca1 Notes MidtermDocument8 pagesPharma Nca1 Notes MidtermAICEL A. ABILNo ratings yet
- Cholinergic Agents: Pharmaceutical Chemistry 2Document64 pagesCholinergic Agents: Pharmaceutical Chemistry 2ahmed hotyNo ratings yet
- Neuropharma AntidementiaDocument29 pagesNeuropharma AntidementiaKeanne Paula AmamanglonNo ratings yet
- Autonomic Nervous System PharmacologyDocument69 pagesAutonomic Nervous System Pharmacologymichot feleguNo ratings yet
- Effects and Uses of Muscarinic Receptor Agonists and AntagonistsDocument21 pagesEffects and Uses of Muscarinic Receptor Agonists and AntagonistsKartikaNo ratings yet
- Anticolinergic Drugs: Mechanisms and UsesDocument26 pagesAnticolinergic Drugs: Mechanisms and UsesHuzaifa KhaleeqNo ratings yet
- Cholinergic Agonists: Dr. Pramod P Bhalerao (M.D.) Asst. Professor Dept. of PharmacologyDocument48 pagesCholinergic Agonists: Dr. Pramod P Bhalerao (M.D.) Asst. Professor Dept. of Pharmacologypramod bhalerao0% (1)
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- Direct Acting Muscarinic AgonistDocument6 pagesDirect Acting Muscarinic AgonistDeia ArahmanNo ratings yet
- Cholinoceptors Activating Drugs.Document48 pagesCholinoceptors Activating Drugs.Kate EvangelistaNo ratings yet
- Drugs in PregnancyDocument14 pagesDrugs in Pregnancypranavibirru96No ratings yet
- Parasympathomimetic DrugsDocument156 pagesParasympathomimetic Drugsjunaid imranNo ratings yet
- Para SympathomimeticsDocument58 pagesPara SympathomimeticsMaha KhalidNo ratings yet
- Outline CH 12 Neuromuscular-Blocking Drugs (NMBDS) and Reversal AgentsDocument36 pagesOutline CH 12 Neuromuscular-Blocking Drugs (NMBDS) and Reversal AgentsCinthia Gonzalez NunezNo ratings yet
- Pharmacology of Autonomic Nervous SystemDocument29 pagesPharmacology of Autonomic Nervous SystemTahir AzizNo ratings yet
- Materi KolinergikDocument62 pagesMateri KolinergikWira KrisnaNo ratings yet
- Pharmacology FirecrackerDocument37 pagesPharmacology FirecrackerRehan Usman100% (1)
- Pcol 1 Ans Midterm PDFDocument9 pagesPcol 1 Ans Midterm PDFJillian Mae DacerNo ratings yet
- 4-Anticholinergic DrugsDocument33 pages4-Anticholinergic DrugsYoueel IbrahemNo ratings yet
- PHARMACOLOGY LECTURES CHOLINERGIC MECHANISMS DR THERESA JOHN Sent To BSC SEP 20 2021Document33 pagesPHARMACOLOGY LECTURES CHOLINERGIC MECHANISMS DR THERESA JOHN Sent To BSC SEP 20 2021Ebenezer SamuelNo ratings yet
- Indirectly Acting Cholinergic DrugsDocument13 pagesIndirectly Acting Cholinergic DrugshariniNo ratings yet
- Anticholinergic AgentsDocument36 pagesAnticholinergic AgentsNicole GalvezNo ratings yet
- 3 CompoundsDocument27 pages3 CompoundsfidhavfathimaNo ratings yet
- Anti Plate Let 2016Document14 pagesAnti Plate Let 2016Desti Ratna PutriNo ratings yet
- Pharmacology of Anaesthetics PDFDocument69 pagesPharmacology of Anaesthetics PDFRanti SapitriNo ratings yet
- SympathomimeticDocument71 pagesSympathomimeticahmad tariqNo ratings yet
- Al-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonDocument42 pagesAl-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonAsdar LeaqerNo ratings yet
- Cholinergic AgonistDocument34 pagesCholinergic AgonistRoma BeygNo ratings yet
- Drugs Acting On Autonomic GangliaDocument9 pagesDrugs Acting On Autonomic GangliaDita Hasni100% (1)
- Cholinergic System: Play A Significant Role in Termination of Acetylcholine's Effect in The SynapseDocument7 pagesCholinergic System: Play A Significant Role in Termination of Acetylcholine's Effect in The SynapseWilliam BufNo ratings yet
- Cholinergic Agonists and AntagonistsDocument750 pagesCholinergic Agonists and AntagonistsClarissa MaglalangNo ratings yet
- TNAHandbook - 9 15 2009 PDFDocument188 pagesTNAHandbook - 9 15 2009 PDFShaukat HayatNo ratings yet
- Listeningppt1 131122090355 Phpapp02Document24 pagesListeningppt1 131122090355 Phpapp02Rodjan MoscosoNo ratings yet
- Bazigar 8Document153 pagesBazigar 8Shaukat Hayat100% (1)
- Inka P-1Document226 pagesInka P-1Shaukat HayatNo ratings yet
- Medicinal PlantsDocument7 pagesMedicinal PlantsamirabuttNo ratings yet
- Industry List of RawalpindiDocument18 pagesIndustry List of RawalpindiShaukat HayatNo ratings yet
- No Littering Day 2012 ReportDocument5 pagesNo Littering Day 2012 ReportShaukat HayatNo ratings yet
- Blood Donors List Zahida Naz MSO Drug A Blood Report (Final)Document18 pagesBlood Donors List Zahida Naz MSO Drug A Blood Report (Final)Shaukat HayatNo ratings yet
- Environment Club PosterDocument1 pageEnvironment Club PosterShaukat HayatNo ratings yet
- RNTCP India - Training Module (Dec - 2010) For Medical OfficersDocument128 pagesRNTCP India - Training Module (Dec - 2010) For Medical OfficersDr.Sagindar100% (1)
- Free Radical Scavenging Activity of Albizia Lebbeck Methanolic Extract in Arthritic RatsDocument8 pagesFree Radical Scavenging Activity of Albizia Lebbeck Methanolic Extract in Arthritic RatsAshik JonaedNo ratings yet
- V EVS Question Bank For SA-1: by Mazumdar Sankar, PRT (SS), AECS, ManuguruDocument41 pagesV EVS Question Bank For SA-1: by Mazumdar Sankar, PRT (SS), AECS, Manuguruspanja_barcNo ratings yet
- Ijwh 218933 Retained Placenta After Vaginal Delivery Risk Factors and M 2Document8 pagesIjwh 218933 Retained Placenta After Vaginal Delivery Risk Factors and M 2terry mutiaNo ratings yet
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- Soal Bahasa Inggris Kls 4 SDDocument2 pagesSoal Bahasa Inggris Kls 4 SDVivin_chepink__566050% (4)
- Patient Assessment: Nabua Fire StationDocument34 pagesPatient Assessment: Nabua Fire Stationkheyan2013No ratings yet
- ANP1105 Final Exam Review - Respiratory, Lymphatic SystemsDocument4 pagesANP1105 Final Exam Review - Respiratory, Lymphatic SystemsVienna GilmoreNo ratings yet
- Malaysia Health Declaration FormDocument3 pagesMalaysia Health Declaration FormMohd ShahrirNo ratings yet
- Gut Microbiome Composition and Role in Digestion & Disease PreventionDocument13 pagesGut Microbiome Composition and Role in Digestion & Disease PreventionAik NoeraNo ratings yet
- 23 How-To-Do-Hardy-Weinberg-ProblemsDocument5 pages23 How-To-Do-Hardy-Weinberg-Problemsapi-241528754No ratings yet
- Introduction To NeuroanatomyDocument14 pagesIntroduction To NeuroanatomyRosalie CalisinNo ratings yet
- Fourth Periodical Exam in 2018Document14 pagesFourth Periodical Exam in 2018robert valdez100% (1)
- Campilobacteriosis BovinaDocument4 pagesCampilobacteriosis BovinaAlmendraNo ratings yet
- Young Talk, July 2010Document4 pagesYoung Talk, July 2010Straight Talk FoundationNo ratings yet
- BloodDocument7 pagesBloodNicol RojasNo ratings yet
- Host Pathogen Interactions: Types, Mechanisms and DefensesDocument18 pagesHost Pathogen Interactions: Types, Mechanisms and DefensesSubbaraoNo ratings yet
- Feline Soft Tissue and General Surgery (VetBooks - Ir)Document721 pagesFeline Soft Tissue and General Surgery (VetBooks - Ir)cosminaNo ratings yet
- 07_Wildemount Gazetteer - Eiselcross - Explorer's Guide to Wildemount - Sources - D&D BeyondDocument13 pages07_Wildemount Gazetteer - Eiselcross - Explorer's Guide to Wildemount - Sources - D&D BeyonddominikNo ratings yet
- Rabies in Children: Bite by Infected Dog Leads to Fatal DiseaseDocument9 pagesRabies in Children: Bite by Infected Dog Leads to Fatal DiseaseIrish AlonzoNo ratings yet
- Module 2Document15 pagesModule 2andreaesp5949555No ratings yet
- Incidents of Foreign Sport and Travel by Colonel PollokDocument504 pagesIncidents of Foreign Sport and Travel by Colonel Pollokcarlpasha1369No ratings yet
- (BẢN TỔNG HỢP) CHUYÊN ĐỀ ÔN TẬP THPT THEO ĐỀ MINH HỌA, FULL KEYDocument65 pages(BẢN TỔNG HỢP) CHUYÊN ĐỀ ÔN TẬP THPT THEO ĐỀ MINH HỌA, FULL KEYnguyenngocbaonhi0108No ratings yet