You might also like
- Pembrolizumab For Previously TreatedDocument11 pagesPembrolizumab For Previously Treatedalex.losadaNo ratings yet
- Kim 2005Document5 pagesKim 2005cristina_zaharia865440No ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- EVIDoa 2200015Document11 pagesEVIDoa 2200015Gustavo BraccoNo ratings yet
- Prognostic Factors in Non-Hodgkin LymphomaDocument8 pagesPrognostic Factors in Non-Hodgkin Lymphomaraio interionfashionNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- Low-Dose Cytarabine Treatment in Elderly AML PatientsDocument7 pagesLow-Dose Cytarabine Treatment in Elderly AML Patientsbryan ruditaNo ratings yet
- Carboplatin-Paclitaxel vs Carboplatin-Pegylated Liposomal Doxorubicin for Platinum-Sensitive Ovarian CancerDocument6 pagesCarboplatin-Paclitaxel vs Carboplatin-Pegylated Liposomal Doxorubicin for Platinum-Sensitive Ovarian Cancerbettzy21No ratings yet
- 247 FullDocument10 pages247 FullMeidianty TandiNo ratings yet
- BR Vs CHOPDocument8 pagesBR Vs CHOPabdullahNo ratings yet
- 1 s2.0 S1083879111002916 MainDocument8 pages1 s2.0 S1083879111002916 MainNunungTriwahyuniNo ratings yet
- Background: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckDocument10 pagesBackground: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckjoitNo ratings yet
- Estey 2020Document73 pagesEstey 2020drToikNo ratings yet
- Annotated BibDocument16 pagesAnnotated Bibapi-542958465No ratings yet
- 1 s2.0 S0006497121069950 MainDocument12 pages1 s2.0 S0006497121069950 MainSALEHA HASSANNo ratings yet
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliNo ratings yet
- Comparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisDocument10 pagesComparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisRicky Cornelius TariganNo ratings yet
- Zhang COR 2022Document12 pagesZhang COR 2022icemoonNo ratings yet
- FDA Approval Summary - Atezolizumab and Durvalumab in Combination With Platinum-Based Chemotherapy in Extensive Stage Small Cell Lung CancerDocument6 pagesFDA Approval Summary - Atezolizumab and Durvalumab in Combination With Platinum-Based Chemotherapy in Extensive Stage Small Cell Lung CancerasdffdsaNo ratings yet
- NO102 08 LambornDocument9 pagesNO102 08 LambornAbhilash VemulaNo ratings yet
- Document 1Document10 pagesDocument 1Haya RihanNo ratings yet
- Natali Zuma BDocument6 pagesNatali Zuma BsarahmooNo ratings yet
- 2018 - Novel Drug Treatments of Progressive RadioiodineRefractory Differentiated Thyroid Cancer-Endocrinol Metab Clin N AmDocument16 pages2018 - Novel Drug Treatments of Progressive RadioiodineRefractory Differentiated Thyroid Cancer-Endocrinol Metab Clin N AmDr Eduardo Henrique - EndocrinologistaNo ratings yet
- How I Treat Newly Diagnosed Chronic Phase CMLDocument9 pagesHow I Treat Newly Diagnosed Chronic Phase CMLDenisse SarabiaNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- Prognostic Factors For Survival of Patients With Glioblastoma: Recursive Partitioning AnalysisDocument9 pagesPrognostic Factors For Survival of Patients With Glioblastoma: Recursive Partitioning AnalysisSungjae AnNo ratings yet
- Researcharticle Open AccessDocument10 pagesResearcharticle Open AccessChairul Nurdin AzaliNo ratings yet
- Biology of Blood and Marrow TransplantationDocument6 pagesBiology of Blood and Marrow TransplantationNazihan Safitri AlkatiriNo ratings yet
- Prognostic Value of Changes in Neutrophil-To-Lymphocyte Ratio (NLR) and PLRDocument6 pagesPrognostic Value of Changes in Neutrophil-To-Lymphocyte Ratio (NLR) and PLRdominguezmariela465No ratings yet
- ScienceDocument1 pageScienceQuique TinocoNo ratings yet
- BMC CancerDocument6 pagesBMC CancerJose Antonio VenacostaNo ratings yet
- Biomedicines 12 00669Document15 pagesBiomedicines 12 00669jamel-shamsNo ratings yet
- Keynote 355Document10 pagesKeynote 355Rocio SolervicensNo ratings yet
- BLOOD - BLD 2022 018546 mmc1Document26 pagesBLOOD - BLD 2022 018546 mmc1Susana RocheNo ratings yet
- Gomella 2009Document8 pagesGomella 2009Evelynππ θσυNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- 1857 FullDocument6 pages1857 FullTahniat AishaNo ratings yet
- Grothey, Metasadyuvantagosto07Document4 pagesGrothey, Metasadyuvantagosto07Francisco BetancourtNo ratings yet
- Outcome of Treatment in Adults With Acute Lymphoblastic Leukemia: Analysis of The LALA-94 TrialDocument22 pagesOutcome of Treatment in Adults With Acute Lymphoblastic Leukemia: Analysis of The LALA-94 TrialJoseph TheThirdNo ratings yet
- Radiotherapy in Mantle Cell Lymphoma A Literature ReviewDocument6 pagesRadiotherapy in Mantle Cell Lymphoma A Literature Review2512505993No ratings yet
- Hyerbaric Oxygenation - Final DraftDocument17 pagesHyerbaric Oxygenation - Final Draftapi-542958465No ratings yet
- BJU International - 2021 - Ravi - Optimal Pathological Response After Neoadjuvant Chemotherapy For Muscle Invasive BladderDocument8 pagesBJU International - 2021 - Ravi - Optimal Pathological Response After Neoadjuvant Chemotherapy For Muscle Invasive BladderMajdNo ratings yet
- FB BerDocument18 pagesFB BeryuliaNo ratings yet
- Atezolizumab Plus Anthracycline-Based Chemotherapy in Metastatic Triple-Negative Breast Cancer: The Randomized, Double-Blind Phase 2b ALICE TrialDocument28 pagesAtezolizumab Plus Anthracycline-Based Chemotherapy in Metastatic Triple-Negative Breast Cancer: The Randomized, Double-Blind Phase 2b ALICE Trialitsasweetlife sosweetNo ratings yet
- 1 s2.0 S000649712061936X MainDocument11 pages1 s2.0 S000649712061936X Mainalhattab tempNo ratings yet
- Journal of Clinical Oncology Volume 32 Number 19 July 2014Document10 pagesJournal of Clinical Oncology Volume 32 Number 19 July 2014ivssonNo ratings yet
- Reuter 2010Document8 pagesReuter 2010Hector Javier BurgosNo ratings yet
- Bortezomib in MCLDocument4 pagesBortezomib in MCLapi-26302710No ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- 148415896sad2 - 73671 73671 IJP ApprovedDocument9 pages148415896sad2 - 73671 73671 IJP ApprovedIndra HedarNo ratings yet
- PIIS0923753419310762Document7 pagesPIIS0923753419310762Kamila MuyasarahNo ratings yet
- AACR 2017 Proceedings: Abstracts 1-3062From EverandAACR 2017 Proceedings: Abstracts 1-3062No ratings yet
- AACR 2017 Proceedings: Abstracts 3063-5947From EverandAACR 2017 Proceedings: Abstracts 3063-5947No ratings yet
- Extended Follow-Up On KEYNOTE-024 Suggests Significant Survival Benefit For Pembrolizumab in Patients With PD-L1 50%, But Unanswered Questions RemainDocument5 pagesExtended Follow-Up On KEYNOTE-024 Suggests Significant Survival Benefit For Pembrolizumab in Patients With PD-L1 50%, But Unanswered Questions RemainasdffdsaNo ratings yet
- UntitledDocument26 pagesUntitledAounAbdellahNo ratings yet
- 5 Years KN024Document15 pages5 Years KN024phojessNo ratings yet
- Cancers 13 01880 v2Document21 pagesCancers 13 01880 v2hop truongvanNo ratings yet
- Efficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S DiseaseDocument6 pagesEfficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S Diseasehusni gunawanNo ratings yet
- Treatment of The Elderly When Cure Is The GoalDocument8 pagesTreatment of The Elderly When Cure Is The GoalCatia AraujoNo ratings yet
- Drugs Used in Otology and Their FormulationsDocument4 pagesDrugs Used in Otology and Their FormulationsAnish RajNo ratings yet
- Anatomy & Physiology Unit 1Document29 pagesAnatomy & Physiology Unit 1Priyanjali SainiNo ratings yet
- Toster And-BeattyDocument2 pagesToster And-BeattyGabrysia MajsikNo ratings yet
- Pharmaceutical Compounding in Portuguese PharmaciesDocument9 pagesPharmaceutical Compounding in Portuguese PharmaciesDomingos MarcosNo ratings yet
- Anti Park I Sonia NoDocument6 pagesAnti Park I Sonia NoiurylindzNo ratings yet
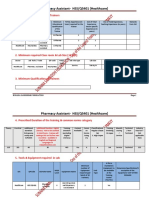
- Pharmacy Assistant-HSS/Q5401 (Healthcare) : 1. Minimum Qualification For TrainersDocument7 pagesPharmacy Assistant-HSS/Q5401 (Healthcare) : 1. Minimum Qualification For TrainersBabar AliNo ratings yet
- Gardner ExhibitDocument8 pagesGardner ExhibitKFORNo ratings yet
- Audi S. (Baker E) Top 100 Drugs - Updated. BJCP 2018Document10 pagesAudi S. (Baker E) Top 100 Drugs - Updated. BJCP 2018rheaNo ratings yet
- Neuroscience NotesDocument35 pagesNeuroscience NotesAnna Conigrave100% (4)
- Dolsten (Mefenamic Acid) : Relief of Pain Including Muscular, Rheumatic, TraumaticDocument2 pagesDolsten (Mefenamic Acid) : Relief of Pain Including Muscular, Rheumatic, TraumaticDavid VillanuevaNo ratings yet
- Neurotransmitter Cheat Sheet AP ReviewDocument2 pagesNeurotransmitter Cheat Sheet AP ReviewNathania DawitNo ratings yet
- Lista BibliográficaDocument17 pagesLista BibliográficafernandaNo ratings yet
- 5 - Antibiotics 2018Document11 pages5 - Antibiotics 2018nae100% (3)
- Appendicitis: Diseases and Conditions: AppendicitisDocument6 pagesAppendicitis: Diseases and Conditions: AppendicitisWen RodsaNo ratings yet
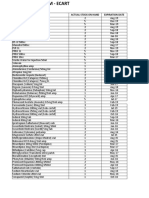
- ER pharmacy inventory levels and expiration datesDocument1 pageER pharmacy inventory levels and expiration datesROSE MERCADONo ratings yet
- (Lecture 3) Vice, Drug Education and ControlDocument18 pages(Lecture 3) Vice, Drug Education and ControlJohnpatrick DejesusNo ratings yet
- 1000 Drug CardsDocument33 pages1000 Drug Cardstfish106588% (90)
- Evaluation of Drug Administration ErrorsDocument8 pagesEvaluation of Drug Administration ErrorsAchmad Indra AwaluddinNo ratings yet
- Medical Uses of Sodium Thiosulfate PDFDocument3 pagesMedical Uses of Sodium Thiosulfate PDFPutri AzzahraNo ratings yet
- Assignment: Importance of Biotransformation in The Human BodyDocument2 pagesAssignment: Importance of Biotransformation in The Human BodyMD REFATNo ratings yet
- Drug Therapy For Gastrointestinal Disease PDFDocument354 pagesDrug Therapy For Gastrointestinal Disease PDFFabrizzio BardalesNo ratings yet
- Maya Biotech Private LimitedDocument21 pagesMaya Biotech Private LimitedRusan PNo ratings yet
- Screenshot 2023-04-26 at 1.31.41 PMDocument1 pageScreenshot 2023-04-26 at 1.31.41 PMRenadNo ratings yet
- General ToxicologyDocument107 pagesGeneral Toxicologynitin tyagiNo ratings yet
- Limba Engleza Business Letters and EmailsDocument11 pagesLimba Engleza Business Letters and EmailsJanosi TimeaNo ratings yet
- Cerebrovascular Accident (Stroke) Drug Study: Submitted By: Daryl S. AbrahamDocument4 pagesCerebrovascular Accident (Stroke) Drug Study: Submitted By: Daryl S. AbrahamBiway RegalaNo ratings yet
- Fourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A SeriesDocument3 pagesFourteen Illustrated Drug Information Booklets: The Truth About Drugs Is A Seriesjoshuaangue60% (5)
- Dokumen - Tips General Pharmacology by DR BashirDocument21 pagesDokumen - Tips General Pharmacology by DR BashirMuhammad WaleedNo ratings yet
- Print 2Document7 pagesPrint 2ridawahyuni09No ratings yet
- Paediatric Drug Computation: Prepared By: Nursing Education Al Rayan HospitalDocument43 pagesPaediatric Drug Computation: Prepared By: Nursing Education Al Rayan HospitalDyan AmisolaNo ratings yet