You might also like
- Dalidig - Drug StudyDocument28 pagesDalidig - Drug StudyRaf DalidigNo ratings yet
- Amiodarone2Document2 pagesAmiodarone2Christine Pialan SalimbagatNo ratings yet
- College of Nursing: Pharmacology Drug StudyDocument2 pagesCollege of Nursing: Pharmacology Drug StudyChristine Pialan SalimbagatNo ratings yet
- AmiodaroneDocument4 pagesAmiodaroneTri Purma SariNo ratings yet
- Final Drug Study-12-25Document41 pagesFinal Drug Study-12-25Poinsithia OrlandaNo ratings yet
- Digoxin Drug StudyDocument2 pagesDigoxin Drug StudyHarline GonzagaNo ratings yet
- P.W Drug Cards Week 10.... REDOOODocument19 pagesP.W Drug Cards Week 10.... REDOOOPRECIOUS wardNo ratings yet
- AmiodaroneDocument4 pagesAmiodaroneChristian Dave EndinoNo ratings yet
- DigoxinDocument4 pagesDigoxinJaessa FelicianoNo ratings yet
- Fangki DS GradedDocument9 pagesFangki DS GradedRod Reynon BorceNo ratings yet
- Drug Study - DigoxinDocument2 pagesDrug Study - DigoxinDanielle AglusolosNo ratings yet
- Emergency DrugsDocument15 pagesEmergency DrugsMikaela Carisse F. BalbonNo ratings yet
- Drug AnalysisDocument9 pagesDrug AnalysisKyle DapulagNo ratings yet
- Mindanao State University - Iligan Institute of Technology Student: Section: 263Document2 pagesMindanao State University - Iligan Institute of Technology Student: Section: 263AkiraMamo100% (1)
- Drug Study (Duty2)Document3 pagesDrug Study (Duty2)Robert َMirandaNo ratings yet
- Clarisse B. Cerame - Drug Study - PsychopharmacologyDocument5 pagesClarisse B. Cerame - Drug Study - PsychopharmacologyClarisse Biagtan CerameNo ratings yet
- Drug Study Sir MarkDocument5 pagesDrug Study Sir MarkKceey CruzNo ratings yet
- AtropineDocument3 pagesAtropineChristian Dave EndinoNo ratings yet
- Drug Study: ND RDDocument5 pagesDrug Study: ND RDBinky Gozun100% (1)
- Dopamine HCLDocument1 pageDopamine HCLIvanne Hisoler100% (3)
- Drug Study Atropine SulfateDocument1 pageDrug Study Atropine Sulfateirhizzp75% (8)
- Drug Study - DRDocument2 pagesDrug Study - DRNicole Arriana ResumaNo ratings yet
- Adenosine: Facial Flushing, SweatingDocument26 pagesAdenosine: Facial Flushing, SweatingAnna Sofia ReyesNo ratings yet
- Emergency DrugsDocument19 pagesEmergency DrugsMean Elepaño50% (2)
- Drug StudyDocument8 pagesDrug StudyApril Sarol67% (3)
- FlecainideDocument3 pagesFlecainideAlexandra AntondyNo ratings yet
- DRug Study PhenytoinDocument1 pageDRug Study Phenytoinmichelle marquezNo ratings yet
- Dig Ox inDocument2 pagesDig Ox inJb_Abarado_7467No ratings yet
- Michael Brian Umali 3A:G6 Classification & BDocument3 pagesMichael Brian Umali 3A:G6 Classification & Bexcel21121No ratings yet
- Drug Study (Amiodarone)Document8 pagesDrug Study (Amiodarone)Justine Conui100% (1)
- Drug StudyDocument4 pagesDrug StudyElva Borlado BilocuraNo ratings yet
- CatapresDocument1 pageCatapresCen Janber CabrillosNo ratings yet
- Case-Scenario-Major Depressive Disorder-BuenconsejoDocument6 pagesCase-Scenario-Major Depressive Disorder-BuenconsejoCarna BuenconsejoNo ratings yet
- Albuterol SulfateDocument1 pageAlbuterol SulfatechristinechaellemorenoNo ratings yet
- Respi Drugs 1Document10 pagesRespi Drugs 1TpdNo ratings yet
- Metoprolol Drug StudyDocument4 pagesMetoprolol Drug StudyCrisha Ann Billones BacutaNo ratings yet
- Drug Study - Carvedilol: Vijandre, Sheryl G. BSN Iii-IDocument2 pagesDrug Study - Carvedilol: Vijandre, Sheryl G. BSN Iii-IJan Emmanuel DC SerranoNo ratings yet
- Drug Study JSGSDocument8 pagesDrug Study JSGSJohannes SantosNo ratings yet
- Gabion drugstudyCKDDocument5 pagesGabion drugstudyCKDShiehan Mae ForroNo ratings yet
- XylocaineDocument1 pageXylocaineRozanne BanzaliNo ratings yet
- Name of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Responsibilities Generic Name: ClassificationDocument4 pagesName of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Responsibilities Generic Name: ClassificationAnalyn Sarmiento100% (1)
- Mindanao State University - Iligan Institute of Technology Student: Egao, Vanessa Jones C. Section: Block 260Document2 pagesMindanao State University - Iligan Institute of Technology Student: Egao, Vanessa Jones C. Section: Block 260Vanessa EgaoNo ratings yet
- Drug Name WPS OfficeDocument2 pagesDrug Name WPS OfficeCAMILLE GAIL HADJIRANINo ratings yet
- Drug Study Valproate SodiumDocument4 pagesDrug Study Valproate SodiumLouie Danielle SegarraNo ratings yet
- Injection, OTC Nasal Solution:: Generic Name: Action: IndicationsDocument8 pagesInjection, OTC Nasal Solution:: Generic Name: Action: IndicationsRonald Anthony TobiasNo ratings yet
- Drug Study 1Document3 pagesDrug Study 1G4 AMOYO ANGELICA NICOLENo ratings yet
- NifedipineDocument3 pagesNifedipineNovi YulianaNo ratings yet
- Generic Name: Ordered: Indications: Contraindications BeforeDocument3 pagesGeneric Name: Ordered: Indications: Contraindications BeforeChenime Añana0% (1)
- Drug StudyDocument27 pagesDrug StudyChan SorianoNo ratings yet
- Schizophrenia DSDocument2 pagesSchizophrenia DSCatungal RophineNo ratings yet
- Forcadilla MedsudrugstudyDocument11 pagesForcadilla MedsudrugstudyKeir Mrls ForcadillaNo ratings yet
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- 2 Assisting Clients To Use Incentive Spirometer DosdosDocument3 pages2 Assisting Clients To Use Incentive Spirometer DosdosBianca Mikaela DosdosNo ratings yet
- 1-Deep Breathing and Cough Exercises - DosdosDocument6 pages1-Deep Breathing and Cough Exercises - DosdosBianca Mikaela DosdosNo ratings yet
- Endorsement NotesDocument2 pagesEndorsement NotesBianca Mikaela DosdosNo ratings yet
- 1ST SceneSpanish Tried To Get St. Michael To OzamisDocument2 pages1ST SceneSpanish Tried To Get St. Michael To OzamisBianca Mikaela DosdosNo ratings yet
- 1st Quarter Summative Assessment Answer SheetDocument1 page1st Quarter Summative Assessment Answer SheetBianca Mikaela DosdosNo ratings yet
- 1 Quarter Reflection and 2 Quarter GoalsDocument2 pages1 Quarter Reflection and 2 Quarter GoalsBianca Mikaela DosdosNo ratings yet
- MSU-Iligan Institute of Technology: Nursing Health Assessment IDocument2 pagesMSU-Iligan Institute of Technology: Nursing Health Assessment IBianca Mikaela DosdosNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- Name: - Date: - Evaluator/Signature: - GradeDocument7 pagesName: - Date: - Evaluator/Signature: - GradeBianca Mikaela DosdosNo ratings yet
- Physical Examination and Review of Systems: Patient's Name / Room No. - 1Document3 pagesPhysical Examination and Review of Systems: Patient's Name / Room No. - 1Bianca Mikaela DosdosNo ratings yet
- Applying A Wet-To-dry DressingDocument4 pagesApplying A Wet-To-dry DressingBianca Mikaela Dosdos0% (1)
- 2nd Appraisal Exam DosdosDocument5 pages2nd Appraisal Exam DosdosBianca Mikaela DosdosNo ratings yet
- Changing A Dry Sterile DressingDocument6 pagesChanging A Dry Sterile DressingBianca Mikaela DosdosNo ratings yet
- Name: - Date: - Evaluator/Signature: - GradeDocument3 pagesName: - Date: - Evaluator/Signature: - GradeBianca Mikaela DosdosNo ratings yet
- Wound Irrigation DefinitionDocument3 pagesWound Irrigation DefinitionBianca Mikaela DosdosNo ratings yet
- Module 3: The Web and The Internet: College of Computer and Information SciencesDocument9 pagesModule 3: The Web and The Internet: College of Computer and Information SciencesBianca Mikaela DosdosNo ratings yet
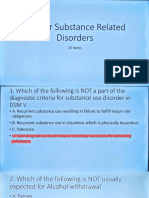
- Psychiatry 3 - Substance Related Disorder MCQsDocument16 pagesPsychiatry 3 - Substance Related Disorder MCQsjsanguenza88No ratings yet
- Regional Anesthetic Blocks - StatPearls - NCBI BookshelfDocument7 pagesRegional Anesthetic Blocks - StatPearls - NCBI BookshelfCarolina SidabutarNo ratings yet
- The 1991 CIA World Factbook by United States. Central Intelligence AgencyDocument1,324 pagesThe 1991 CIA World Factbook by United States. Central Intelligence AgencyGutenberg.org100% (1)
- Muscle-Brain Communication in Pain The Key Role of MyokinesDocument11 pagesMuscle-Brain Communication in Pain The Key Role of MyokinesGrossl Schorr FernandoNo ratings yet
- 2022 HRS - Aggressive B-Cell Lymphomas FINALDocument80 pages2022 HRS - Aggressive B-Cell Lymphomas FINALИван НегарэNo ratings yet
- Resume Radhika KDocument1 pageResume Radhika KJenniferNo ratings yet
- Principles of HemodynamicDocument48 pagesPrinciples of HemodynamicdevdsantoshNo ratings yet
- Mapping Data KFA - 20230119Document2,003 pagesMapping Data KFA - 20230119RSKB Islam CawasNo ratings yet
- Eugenol - WikipediaDocument9 pagesEugenol - WikipediaYudha Sanditya SaputraNo ratings yet
- Treated Like A Simpleton by Medical OfficerDocument2 pagesTreated Like A Simpleton by Medical OfficerKelly LeeNo ratings yet
- Apotek Agung Medika Farma: Jalan Ki Warsiki Blok Ki Buyut Desa Kedungdalem Gegesik - Kabupaten CirebonDocument10 pagesApotek Agung Medika Farma: Jalan Ki Warsiki Blok Ki Buyut Desa Kedungdalem Gegesik - Kabupaten CirebonagungNo ratings yet
- 5.nervous System PDFDocument88 pages5.nervous System PDFMelancholy MedicineNo ratings yet
- Adherence and Quality of Life Among Diabetic Patients With HypertensionDocument6 pagesAdherence and Quality of Life Among Diabetic Patients With HypertensionIJPHSNo ratings yet
- Pathophysiology 2nd YearDocument55 pagesPathophysiology 2nd YeartiffylolaNo ratings yet
- Curcuma Longa Extract.: ActionDocument2 pagesCurcuma Longa Extract.: ActionDrShiva PrasadNo ratings yet
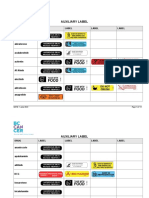
- Auxiliary Label LISTDocument14 pagesAuxiliary Label LISTAbdur RachmanNo ratings yet
- Nicotine - It May Have A Good Side - Harvard HealthDocument3 pagesNicotine - It May Have A Good Side - Harvard HealthzimkoNo ratings yet
- ND RDDocument10 pagesND RDOdyNo ratings yet
- Theophylline: Yeli Pandu Gustia 0811012071Document31 pagesTheophylline: Yeli Pandu Gustia 0811012071Yeli Pandu Gustia100% (1)
- College of Nursing: Cebu Normal UniversityDocument5 pagesCollege of Nursing: Cebu Normal UniversityChelsea WuNo ratings yet
- Antibiotic GuidelineDocument11 pagesAntibiotic GuidelineSanjay ShresthaNo ratings yet
- Psychotropic Drugs.Document15 pagesPsychotropic Drugs.Xiaoqing SongNo ratings yet
- Calcium Channel BlockersDocument2 pagesCalcium Channel BlockersBrittany RamirezNo ratings yet
- COVID 19 and Ischemic Stroke: Mechanisms of Hypercoagulability (Review)Document13 pagesCOVID 19 and Ischemic Stroke: Mechanisms of Hypercoagulability (Review)Martha OktaviaNo ratings yet
- Paracetamol Drug StudyDocument1 pageParacetamol Drug StudyArthur Christopher CorpuzNo ratings yet
- Clinical EfficacyDocument6 pagesClinical EfficacyNurRahmah'amma'HasanuddinNo ratings yet
- T1K UpdateDocument24 pagesT1K UpdateolivenanaNo ratings yet
- PHAR635 Parenteral Dosage Forms: Instructors: Dr. Tarek Jenani Dr. Faten HamedDocument29 pagesPHAR635 Parenteral Dosage Forms: Instructors: Dr. Tarek Jenani Dr. Faten HamedundeadrebornNo ratings yet
- Gerd - Peptic Ulcer - GastritisDocument87 pagesGerd - Peptic Ulcer - GastritisErickson V. LibutNo ratings yet
- Blanko LPLPO PustuDocument7 pagesBlanko LPLPO Pustuagus fathaniNo ratings yet