You might also like
- MetildopaDocument6 pagesMetildopasistri ajeng gmNo ratings yet
- Antidyslipidemic Drugs (Geppetti)Document32 pagesAntidyslipidemic Drugs (Geppetti)Ariel OlshevskyNo ratings yet
- Diabetes Case PresentationDocument3 pagesDiabetes Case Presentationdeb haart100% (1)
- Famasi IIDocument6 pagesFamasi IIMerlyn AngelicaNo ratings yet
- AH PharmaII v2Document35 pagesAH PharmaII v2bankai2992No ratings yet
- Therapeutics Question (DKA) : Answer For Q1Document4 pagesTherapeutics Question (DKA) : Answer For Q1Daniel YongNo ratings yet
- Methyldopa Drug StudyDocument2 pagesMethyldopa Drug Studymilkv100% (14)
- AcetazolamideDocument4 pagesAcetazolamideAmarnath SahNo ratings yet
- IRIS 2009 Treatment Recommendations SummaryDocument5 pagesIRIS 2009 Treatment Recommendations SummaryJessicaHernandezNo ratings yet
- DMARD'sDocument9 pagesDMARD'sterencedszaNo ratings yet
- Aki and CKD Therapy 2021Document46 pagesAki and CKD Therapy 2021Alfathri YunediNo ratings yet
- Diuretics: Generic Name: FUROSEMIDEDocument12 pagesDiuretics: Generic Name: FUROSEMIDEJR BetonioNo ratings yet
- Obat Lipidemik: Dept of Pharmacology and Therapeutics FK Undip Oktober, 2018Document38 pagesObat Lipidemik: Dept of Pharmacology and Therapeutics FK Undip Oktober, 2018KaroniNo ratings yet
- Other Diuretics Final 2017Document4 pagesOther Diuretics Final 2017Anonymous sSuBudwdNo ratings yet
- Summary of Product Characteristics 1 Name of The Medicinal ProductDocument9 pagesSummary of Product Characteristics 1 Name of The Medicinal Productddandan_2No ratings yet
- Antihypertensive Drugs - Classification and SynthesisDocument14 pagesAntihypertensive Drugs - Classification and SynthesisCường NguyễnNo ratings yet
- hYPO DRUGDocument17 pageshYPO DRUGpabitraNo ratings yet
- METFORMIN FOR DIABETESDocument13 pagesMETFORMIN FOR DIABETESAllan DiazNo ratings yet
- Approach ConsiderationsDocument5 pagesApproach ConsiderationsGunawan SetiawanNo ratings yet
- Lowers Abnormal Lipid LevelsDocument34 pagesLowers Abnormal Lipid Levelschelle_morales260% (1)
- EE Tarek Exam Hints 2019-1Document83 pagesEE Tarek Exam Hints 2019-1Ibrahim Sayed AhmedNo ratings yet
- Hyperlipedemia PPDocument51 pagesHyperlipedemia PPrabarNo ratings yet
- Dr. Drg. Nur Permatasari, MS. Dr. Dian Nugrahenny, M.BiomedDocument24 pagesDr. Drg. Nur Permatasari, MS. Dr. Dian Nugrahenny, M.BiomedTutde SedanaNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- How Is Hypokalaemia Treated in Adults?: Medicines Q&AsDocument6 pagesHow Is Hypokalaemia Treated in Adults?: Medicines Q&AsNotForAbuseNo ratings yet
- Lipitor: (Atorvastatin Calcium) TabletsDocument29 pagesLipitor: (Atorvastatin Calcium) TabletsEvelinaĐulbićNo ratings yet
- Endo MRCGP 2015Document221 pagesEndo MRCGP 2015AlexandraOsmanNo ratings yet
- Agents Used in Dyslipidemia Chapter Summary - MedecieloDocument3 pagesAgents Used in Dyslipidemia Chapter Summary - MedecieloMEDECIELO MELONo ratings yet
- Diabetes Mellitus: (DM)Document84 pagesDiabetes Mellitus: (DM)Andika HNo ratings yet
- MetFormin Generic Health TabDocument9 pagesMetFormin Generic Health TabNur Ekayani SyamNo ratings yet
- Lipid Lowering AngentDocument22 pagesLipid Lowering AngentDave BraveNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Complications of Diabetes MellitusDocument76 pagesComplications of Diabetes MellitusfrankNo ratings yet
- Syndrome of Inappropriate Adh Secretion (Siadh) PathophysiologyDocument2 pagesSyndrome of Inappropriate Adh Secretion (Siadh) PathophysiologyJuliana FeronNo ratings yet
- CBD DMDocument8 pagesCBD DMEtsubdink HailuNo ratings yet
- Metabolism of methyldopa inside the human bodyDocument4 pagesMetabolism of methyldopa inside the human bodyمحمد حميد عطيةNo ratings yet
- Hypertension: Increase in Blood PressureDocument29 pagesHypertension: Increase in Blood PressureKeesha Mae AnteNo ratings yet
- Indapamid SR Pliva 15 MG Tablete S Produljenim Oslobadjanjem SPCDocument10 pagesIndapamid SR Pliva 15 MG Tablete S Produljenim Oslobadjanjem SPCDuje ErcegovicNo ratings yet
- Brand Names: Generic NameDocument3 pagesBrand Names: Generic NameEzraManzanoNo ratings yet
- Anti Hyperlipidemic Agent PDFDocument11 pagesAnti Hyperlipidemic Agent PDFStefanus Surya100% (1)
- Normopresan Product Characteristics SummaryDocument7 pagesNormopresan Product Characteristics SummaryasdwasdNo ratings yet
- The Cardiovascular System: Classification of AntihypertensivesDocument57 pagesThe Cardiovascular System: Classification of AntihypertensivesDr. Hashibu SsekweyamaNo ratings yet
- 8 Drug StudyDocument19 pages8 Drug StudyLoyloy D ManNo ratings yet
- 2nd - Semester.lecture 3.1-Drugs Used in HypertensionDocument40 pages2nd - Semester.lecture 3.1-Drugs Used in HypertensionToader SilviaNo ratings yet
- PASSMEDICINE MCQs-PHARMACOLOGYDocument107 pagesPASSMEDICINE MCQs-PHARMACOLOGYMohammad Saleh100% (1)
- Emergency DrugsDocument5 pagesEmergency DrugsArra PlacidesNo ratings yet
- Amdocal Final PDFDocument5 pagesAmdocal Final PDFSaifur Rahman SuzonNo ratings yet
- Lipid Management Guidelines Focus on Absolute CVD Risk, LDL ReductionDocument6 pagesLipid Management Guidelines Focus on Absolute CVD Risk, LDL ReductionemirkurtalicNo ratings yet
- Cardiology Pharmacology Review: HMG-CoA Reductase Inhibitors MechanismDocument74 pagesCardiology Pharmacology Review: HMG-CoA Reductase Inhibitors Mechanismshannon_marrero_1No ratings yet
- Interaksi ObatDocument12 pagesInteraksi ObatIai Kepulauan RiauNo ratings yet
- Drug-induced liver injury causes and agentsDocument5 pagesDrug-induced liver injury causes and agentsospapNo ratings yet
- Managing Hyperkalemia in CKD PatientsDocument8 pagesManaging Hyperkalemia in CKD PatientsPratik TripathiNo ratings yet
- Drug StudyDocument10 pagesDrug StudyFranco ObedozaNo ratings yet
- Drug-Study MethyldopaDocument4 pagesDrug-Study MethyldopamayangernszNo ratings yet
- Endocrine Dr. RehabDocument65 pagesEndocrine Dr. RehabMohammed Saad NabhanNo ratings yet
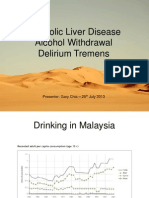
- Alcoholic Liver Disease Alcohol Withdrawal Delirium TremensDocument60 pagesAlcoholic Liver Disease Alcohol Withdrawal Delirium Tremensgarychia100% (1)
- Metformin: Dosing & UsesDocument8 pagesMetformin: Dosing & UsesMaria Alejandra Siachoque JaraNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Nsaids May Cause Rare Kidney Problems in Unborn Babies: Drug Facts LabelsDocument9 pagesNsaids May Cause Rare Kidney Problems in Unborn Babies: Drug Facts LabelsHadi AminiNo ratings yet
- Cirrosis Hepatica DescompensadaDocument55 pagesCirrosis Hepatica DescompensadaJefferson Diaz100% (1)
- Mefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Document20 pagesMefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Riska AuliahNo ratings yet
- Adalat CC (Nifedipine) Extended Release Tablets: For Oral UseDocument15 pagesAdalat CC (Nifedipine) Extended Release Tablets: For Oral UseRiska AuliahNo ratings yet
- Riska Auliah Anjarwati PDFDocument6 pagesRiska Auliah Anjarwati PDFRiska AuliahNo ratings yet
- The Passive VoiceDocument16 pagesThe Passive VoiceMuhammad HaekalNo ratings yet
- Riska Auliah AnjarwatiDocument6 pagesRiska Auliah AnjarwatiRiska AuliahNo ratings yet
- The First 8 Tense ExercisesDocument3 pagesThe First 8 Tense ExercisesRiska AuliahNo ratings yet
- TENSES GUIDEDocument1 pageTENSES GUIDERiska AuliahNo ratings yet
- Subject Verb/Predicate Object ModifierDocument1 pageSubject Verb/Predicate Object ModifierRiska AuliahNo ratings yet
- The First 8 Tense ExercisesDocument3 pagesThe First 8 Tense ExercisesRiska AuliahNo ratings yet
- Hypertension Therapy Guide for Managing Blood PressureDocument69 pagesHypertension Therapy Guide for Managing Blood Pressurerisma sakti pNo ratings yet
- Prevention and Treatment of Systemic Glucocorticoid Side EffectsDocument10 pagesPrevention and Treatment of Systemic Glucocorticoid Side EffectsMahmoud DiaaNo ratings yet
- p200 Magdy McVeigh IndraratnaDocument5 pagesp200 Magdy McVeigh IndraratnaAmmarersNo ratings yet
- Katzung End of Chapter Questions-ModifiedDocument110 pagesKatzung End of Chapter Questions-ModifiedLicensed to Heal0% (1)
- Antihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDocument6 pagesAntihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDwie SeptivianieNo ratings yet
- 11. 201909 抗高血压 antihypertensionDocument72 pages11. 201909 抗高血压 antihypertensionShanon LimNo ratings yet
- Chapter 51 - Diuretic AgentsDocument11 pagesChapter 51 - Diuretic AgentsJonathon100% (2)
- Maharashtra Board Pharmacology Model AnswerDocument19 pagesMaharashtra Board Pharmacology Model AnswerJyoti MangtaniNo ratings yet
- Pharmacology QuestionsDocument33 pagesPharmacology QuestionsPurnimaNo ratings yet
- Hypertension Treatment Steps For HypertensionDocument15 pagesHypertension Treatment Steps For Hypertensionfreelancer08100% (1)
- All McQs PDFDocument524 pagesAll McQs PDFMueen mohsinNo ratings yet
- 4,5,6 - Diuretic PDFDocument27 pages4,5,6 - Diuretic PDFHely PatelNo ratings yet
- Atacand Plus 16/12.5 mg tablets summary of product characteristicsDocument25 pagesAtacand Plus 16/12.5 mg tablets summary of product characteristicsddandan_2No ratings yet
- Guidelines TX of HPNDocument3 pagesGuidelines TX of HPNjheyfteeNo ratings yet
- Laporan Kasus GastroenteritisDocument7 pagesLaporan Kasus GastroenteritisinaNo ratings yet
- Berra 2020Document12 pagesBerra 2020Indri AswariNo ratings yet
- DIURETICSDocument55 pagesDIURETICSRAVISHNo ratings yet
- Hypertension Treatment Steps For HypertensionDocument14 pagesHypertension Treatment Steps For Hypertensiontri setyo bayuajiNo ratings yet
- Diuretics: An Overview of How They Work and Their ClassificationDocument74 pagesDiuretics: An Overview of How They Work and Their Classificationm1k0e100% (1)
- CVS - DiureticsDocument8 pagesCVS - Diureticshlouis8No ratings yet
- Pharmacotherapy of HypertensionDocument90 pagesPharmacotherapy of HypertensionJambo BuneNo ratings yet
- AHA JNC 8 GuidelineDocument12 pagesAHA JNC 8 GuidelineFamidur RsNo ratings yet
- AV Y TẾ 2Document27 pagesAV Y TẾ 2Đạt Bùi TiếnNo ratings yet
- Diuretic Drugs: TEACH For Nurses ForDocument9 pagesDiuretic Drugs: TEACH For Nurses ForLouwella RamosNo ratings yet
- DiureticsDocument10 pagesDiureticsAyla NacariøNo ratings yet
- Diuretics 140628134114 Phpapp02Document45 pagesDiuretics 140628134114 Phpapp02P merugu100% (1)
- Antihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmDocument6 pagesAntihypertensive Drugs: Re Jackson BSC MB CHB Frca and MC Bellamy MB BS MA FRCA FRCP (Edin) FficmAndreas SmfNo ratings yet
- Diuretics TableDocument5 pagesDiuretics TableLaylee ClareNo ratings yet
- DiPette Et Al-2019-The Journal of Clinical HypertensionDocument12 pagesDiPette Et Al-2019-The Journal of Clinical HypertensionDenise GuevaraNo ratings yet
- Pharmacology HandoutDocument84 pagesPharmacology Handoutnanashimii100% (4)