You might also like
- 1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death LectureDocument25 pages1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death Lectureregeti bhargavNo ratings yet
- 2.2. Cell Adaptation, Injury and DeathDocument53 pages2.2. Cell Adaptation, Injury and Deathakoeljames8543No ratings yet
- PathologyDocument119 pagesPathologyDavid VijayNo ratings yet
- Cell Adaptation, Injury and DeathDocument91 pagesCell Adaptation, Injury and DeathAmera ElsayedNo ratings yet
- Histopathlogy General Concept Part 1Document58 pagesHistopathlogy General Concept Part 1Kimberly AnnNo ratings yet
- Conference 1Document71 pagesConference 1titusonNo ratings yet
- AnticancerDocument78 pagesAnticancerRajkishor GogoiNo ratings yet
- Chapter03 Altered Cell & TissueDocument54 pagesChapter03 Altered Cell & Tissuechris100% (1)
- Apoptosis & Necrosis: Suad Omar NafiDocument46 pagesApoptosis & Necrosis: Suad Omar Nafisoad onafiNo ratings yet
- CellularAdaptation Injury and Death - General OverviewDocument13 pagesCellularAdaptation Injury and Death - General OverviewlydNo ratings yet
- Anatomy Revised and Extended Copy - 39 BCSDocument48 pagesAnatomy Revised and Extended Copy - 39 BCSAjob ArafatNo ratings yet
- ReviewDocument102 pagesReviewAbir AlamNo ratings yet
- Cellular Adaptation - 2022Document49 pagesCellular Adaptation - 2022Leo Lucifer 104No ratings yet
- Anticancer DrugsDocument41 pagesAnticancer DrugsMehran RiazNo ratings yet
- Cell Injury and AdaptationDocument47 pagesCell Injury and AdaptationPujashree SabatNo ratings yet
- Altered Cell Biology: PathophysiologyDocument33 pagesAltered Cell Biology: PathophysiologyNi CaoNo ratings yet
- Pathology01 CellDeath Inflammation RepairDocument140 pagesPathology01 CellDeath Inflammation RepairMiguel AranaNo ratings yet
- Pengantar Patologi AnatomiDocument47 pagesPengantar Patologi AnatomiChristian V. H. TambaNo ratings yet
- Cell Cycle in Health and DiseaseDocument26 pagesCell Cycle in Health and DiseaseandiswulandariNo ratings yet
- General Pathology - Lecture 1 SlideshowDocument82 pagesGeneral Pathology - Lecture 1 SlideshowLily Dawn Marquez JoloNo ratings yet
- Cell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument27 pagesCell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PAlindaNo ratings yet
- 1 Introduction and Cell AdaptationDocument142 pages1 Introduction and Cell AdaptationyuyanwongNo ratings yet
- 010 Principios Generales de La Terapia Antitumoral. Antimetabolitos IDocument118 pages010 Principios Generales de La Terapia Antitumoral. Antimetabolitos IManuel Alberto Toledo DaviaNo ratings yet
- Cell Injury and Adaptation: Fort SalvadorDocument44 pagesCell Injury and Adaptation: Fort SalvadorFort SalvadorNo ratings yet
- PathologyDocument117 pagesPathologyDrChauhanNo ratings yet
- Types of Cell DeathDocument7 pagesTypes of Cell DeathRutvi ChovatiyaNo ratings yet
- Carcinogenesis: Tee L. GuidottiDocument21 pagesCarcinogenesis: Tee L. GuidottiLhyne PablicoNo ratings yet
- PathologyDocument217 pagesPathologyhindrina8No ratings yet
- Adaptations, Cell Injury, Cell Death: Dr. Ashish Jawarkar, MDDocument77 pagesAdaptations, Cell Injury, Cell Death: Dr. Ashish Jawarkar, MDEdsel Ian S. FuentesNo ratings yet
- Neoplasia 1 What Is A Tumour?: Leicester Warwick Medical SchoolDocument42 pagesNeoplasia 1 What Is A Tumour?: Leicester Warwick Medical SchoolDaniel Triana HNo ratings yet
- Anti-Neoplastic Drugs-1Document79 pagesAnti-Neoplastic Drugs-1Aahad AmeenNo ratings yet
- Histopathology General Concept Part 2Document50 pagesHistopathology General Concept Part 2Kimberly AnnNo ratings yet
- Plenary 2: "Yang Tersembunyi"Document92 pagesPlenary 2: "Yang Tersembunyi"Fathoni akbarNo ratings yet
- FINALS Session 12 Gene TherapyDocument40 pagesFINALS Session 12 Gene TherapyEunice VillacacanNo ratings yet
- 02.07.4 Cell Injury I FINALDocument52 pages02.07.4 Cell Injury I FINALNawlannieNo ratings yet
- Cancer Biology 2023Document82 pagesCancer Biology 2023STACEY SALVILLANo ratings yet
- Cellular Response To Stress & Toxic Insults: Adaptation, Injury & DeathDocument70 pagesCellular Response To Stress & Toxic Insults: Adaptation, Injury & DeathMila DamayantiNo ratings yet
- 59 Genetics of Cancer II Tumor Suppressors and ApoptosisDocument68 pages59 Genetics of Cancer II Tumor Suppressors and ApoptosisLunaLureNo ratings yet
- Molecular OncogenesIsDocument126 pagesMolecular OncogenesIslowellaNo ratings yet
- Enabling Invasion and MetastasisDocument3 pagesEnabling Invasion and MetastasisAsish GeiorgeNo ratings yet
- Cell InjuryDocument48 pagesCell InjurySALWA ASHFIYA -No ratings yet
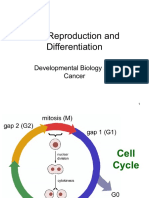
- 05 - Cell Reproduction and DifferentiationDocument14 pages05 - Cell Reproduction and DifferentiationTius LenaNo ratings yet
- Cell Cycle in Health and DiseaseDocument27 pagesCell Cycle in Health and DiseaseAmalia DeviNo ratings yet
- Nursing 404 Normal and Abnormal Human Physiology: CancerDocument47 pagesNursing 404 Normal and Abnormal Human Physiology: CancerPnpplorangeNo ratings yet
- Necrosis and Cellualr AdaptationDocument56 pagesNecrosis and Cellualr AdaptationEs SarveshNo ratings yet
- Patofisiologi Kanker OkDocument79 pagesPatofisiologi Kanker OkleilaNo ratings yet
- ETIOLOGY of Cell InjuryDocument77 pagesETIOLOGY of Cell InjurybesthachakrapaniNo ratings yet
- Cell Injury, Cell Death, AdaptationDocument64 pagesCell Injury, Cell Death, Adaptationtiararudianti20No ratings yet
- Intercellular Communications & ApoptosisDocument26 pagesIntercellular Communications & ApoptosisAjinkya AravindNo ratings yet
- The HallMarks of CancerDocument33 pagesThe HallMarks of CancerAmaan Khan100% (1)
- CH1 Path D&R AgamDocument34 pagesCH1 Path D&R Agam062100% (1)
- Session 3Document76 pagesSession 3kasper mkNo ratings yet
- Genetika Molekuler NeoplasmaDocument23 pagesGenetika Molekuler NeoplasmaAndikaChandraNo ratings yet
- Leucemia Pathophysiology AND Therapy StrategyDocument41 pagesLeucemia Pathophysiology AND Therapy Strategydevi wahyuniNo ratings yet
- 5) Degeneration, Necrosis and GangreneDocument72 pages5) Degeneration, Necrosis and GangreneMadhulikaNo ratings yet
- Cell Injury 2018Document56 pagesCell Injury 2018Mihaela IurescuNo ratings yet
- Neoplasms What Is A Tumor? ClonalityDocument2 pagesNeoplasms What Is A Tumor? ClonalityRosey WhtNo ratings yet
- Hallmarks of Cancer: DR Arnab Kalita PG Fellow Head Neck Oncology BbciDocument40 pagesHallmarks of Cancer: DR Arnab Kalita PG Fellow Head Neck Oncology BbciArnab KalitaNo ratings yet
- Wound Healing, Tissue Repair, and FibrosisDocument28 pagesWound Healing, Tissue Repair, and FibrosisRibka Theodora100% (1)
- Stem Cells in Regenerative Medicine: Carpe Diem – Carpe Vitam!From EverandStem Cells in Regenerative Medicine: Carpe Diem – Carpe Vitam!Rating: 2.5 out of 5 stars2.5/5 (3)
- STS Topic 11 GMOsDocument22 pagesSTS Topic 11 GMOsiblaze2003No ratings yet
- Characterization of HSP27 Phosphorylation Induced by Microtubule Interfering Agents: Implication of p38 Signalling PathwayDocument7 pagesCharacterization of HSP27 Phosphorylation Induced by Microtubule Interfering Agents: Implication of p38 Signalling PathwayEva Del ValleNo ratings yet
- CV - Christoph - Pittius - CV - 2011 PDFDocument3 pagesCV - Christoph - Pittius - CV - 2011 PDFonynhoNo ratings yet
- Biotechnology A Problem ApproachDocument223 pagesBiotechnology A Problem ApproachPathifnder Publication93% (46)
- Micropropagación de Glossonema VariansDocument16 pagesMicropropagación de Glossonema VariansmatateteNo ratings yet
- A Systemic Review Covid-19 VaccineDocument13 pagesA Systemic Review Covid-19 VaccineIJAR JOURNALNo ratings yet
- Halotag Technology: Focus On Imaging: Technical ManualDocument43 pagesHalotag Technology: Focus On Imaging: Technical ManualMoritz ListNo ratings yet
- Biopharming: PHA 758 Biomanufacturing in Pharmaceutical Development of DrugsDocument33 pagesBiopharming: PHA 758 Biomanufacturing in Pharmaceutical Development of DrugsFatina HatoumNo ratings yet
- Lesson Plan Recombinant DNA/Grade 12 B Biology: - Applications 9eDocument4 pagesLesson Plan Recombinant DNA/Grade 12 B Biology: - Applications 9ePutri ApriliyaniNo ratings yet
- Earth and Life Science: Quarter 2 - Module 11: Genetic EngineeringDocument22 pagesEarth and Life Science: Quarter 2 - Module 11: Genetic EngineeringElvin Sajulla BulalongNo ratings yet
- Example Clinical Lab 04.21.2022 PDFDocument4 pagesExample Clinical Lab 04.21.2022 PDFBenziy JijyNo ratings yet
- Evidencia 1 - AbstractDocument3 pagesEvidencia 1 - AbstractPamela OsunzaNo ratings yet
- Seminar IDocument43 pagesSeminar Ikasahun AmareNo ratings yet
- Mark Scheme (Results) January 2022Document16 pagesMark Scheme (Results) January 2022윤소리No ratings yet
- Transposon in MaizeDocument11 pagesTransposon in MaizeSurachat TangpranomkornNo ratings yet
- 2016 Genes and Athletic Performance An UpdateDocument15 pages2016 Genes and Athletic Performance An UpdateFrancisco Antonó Castro WeithNo ratings yet
- ICH Topic Q 6 BDocument17 pagesICH Topic Q 6 BAprianaRohmanNo ratings yet
- Pmecx Avulso 1Document391 pagesPmecx Avulso 1Victor RoticivNo ratings yet
- Hyderabad Database BackupDocument7 pagesHyderabad Database BackupSyed AyazNo ratings yet
- Intl Service For The Acquisition of Agri-Biotech Applications v. Greenpeace - G.R. No. 209271Document19 pagesIntl Service For The Acquisition of Agri-Biotech Applications v. Greenpeace - G.R. No. 209271Ash SatoshiNo ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- Animal Biotechnology Dylan Ayekpam 2167015Document3 pagesAnimal Biotechnology Dylan Ayekpam 2167015SüzShñtä ÅykpmNo ratings yet
- Alkylating AgentsDocument3 pagesAlkylating AgentsIna SimacheNo ratings yet
- 5 Experiments in BiochemistryDocument5 pages5 Experiments in BiochemistrySCIENCE Benjie AvecillaNo ratings yet
- GPAT Biotechemistry SyllabusDocument2 pagesGPAT Biotechemistry Syllabuskumar HarshNo ratings yet
- Biology A Level Handbook 2023Document34 pagesBiology A Level Handbook 2023uzair madanessNo ratings yet
- Potential - Best Compatibility ModeDocument14 pagesPotential - Best Compatibility ModeDivya TripathyNo ratings yet
- Aneesh Recommendation 16Document2 pagesAneesh Recommendation 16Aleem MuhammadNo ratings yet
- Biofilms in EntDocument4 pagesBiofilms in EntDrsiya MedfriendNo ratings yet
- Anti-Inflammatory Nutraceuticals and Chronic Diseases: Subash Chandra Gupta Sahdeo Prasad Bharat B. Aggarwal EditorsDocument479 pagesAnti-Inflammatory Nutraceuticals and Chronic Diseases: Subash Chandra Gupta Sahdeo Prasad Bharat B. Aggarwal EditorsRora11100% (1)